
Wound repair of the pretibial and forearm regions presents a challenge during dermatologic surgery as these areas are under significant tension and exhibit increased skin fragility. Various methodologies have been proposed for the closure and repair of such wounds, however, the use of the bilayered suture technique may be simpler and more effective than other techniques such as the pinch stitch, pully stitch, slip-knot stitch, pulley set-back dermal suture, horizontal mattress suture, pully stitch, and tandem pulley stitch. The authors objective was to describe a novel method for the repair of pretibial and forearm wounds following Mohs micrographic surgery utilizing bilayered closure followed by tissue adhesive application.
INTRODUCTION
Wound repair in particular areas of the body presents treatment challenges. Epidermal fragility, inflamed margins, and heightened skin tension secondary to suturing, increase the risk of wound dehiscence and delay healing. Friable tissue is also more likely to be torn by the sutures themselves. No gold standard currently exists for the treatment of pretibial or forearm wound defects. Several techniques have been proposed within the literature including the use of Steri-StripsTM and sutures on linear lacerations,1 in addition to suturing (with Adhesive Retention Suture device) followed by fixative application.2 There are no previously reported management regimens, however, that involve the use of bilayered closure and liquid adhesive.
METHODS
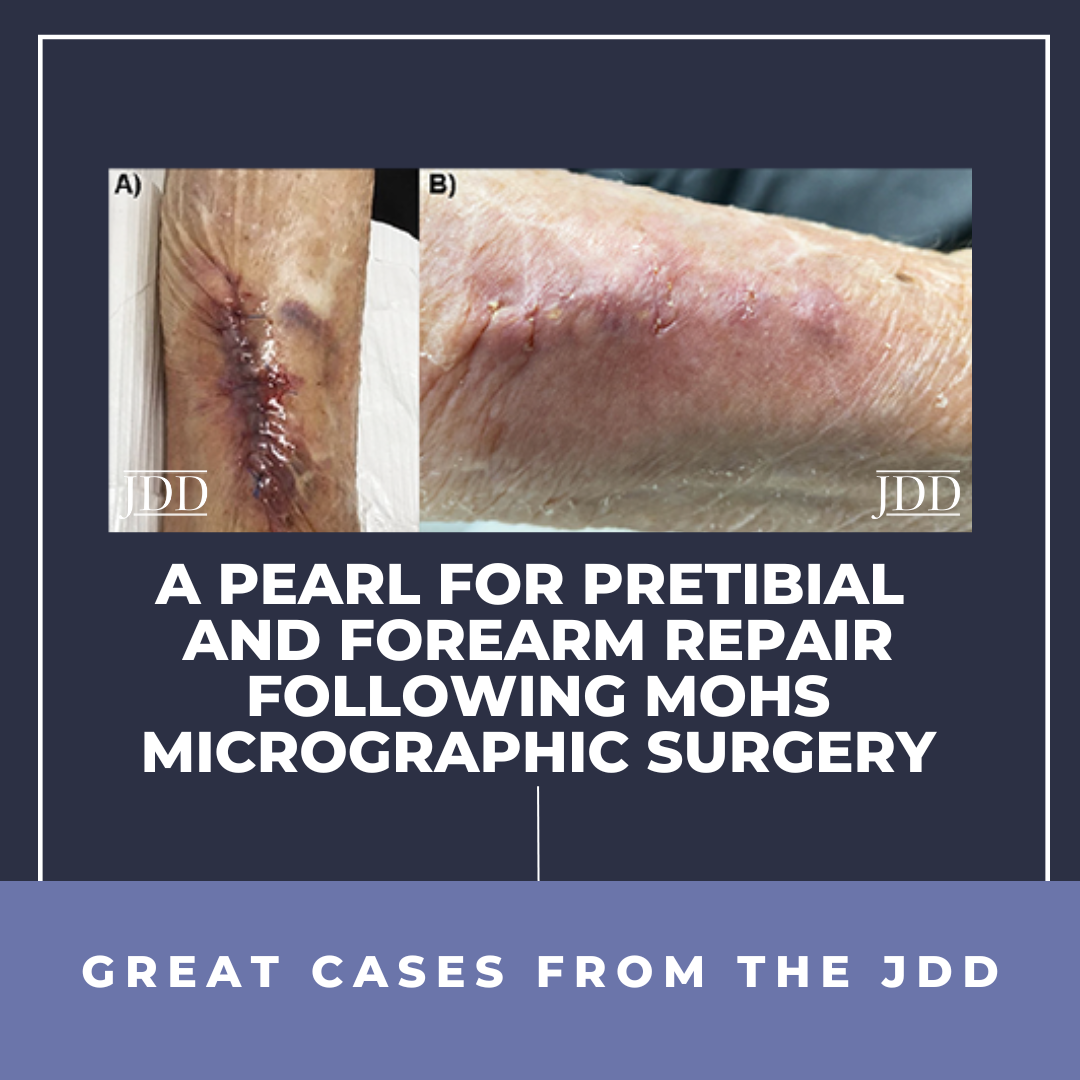
A bilayered suture technique was devised for pretibial and forearm wound closure following Mohs micrographic surgery. The patient’s wounds are cleaned after the procedure using chlorhexidine. The wound is approximated using a 3.0 nylon pulley suture. To decrease wound tension, it can be left in place or removed when the closure, using 3-0 interrupted polyglactin 910 sutures for the subcutaneous layer and interrupted 3-0 nylon sutures for the epidermal layers, is completed. Dermabond (Ethicon) or Mastisol (Ferndale) are subsequently applied to the linear closure and surrounding skin (Figure 1A). Once the adhesive dries, a pressure bandage is applied. Lastly, sutures are removed and the surgical site is assessed at 3 weeks follow-up (Figure 1B). Bilayered closure, then tissue adhesive application, an innovative method for pretibial and forearm wound closure after Mohs surgery, decreases superficial dehiscence and allows for adequate wound healing and approximation. The use of adhesive with this technique helps to prevent the skin

from being torn apart with suture tensions, and the sutures from ripping through the friable skin with tension, or inflammation/edema in the early stages of wound healing. In our experience, this is an easy, safe, accessible method to close pretibial and forearm wounds, under tension, and provides a valuable teaching lesson for dermatology residents and fellows.3
DISCLOSURES
The authors have no conflicts of interest or funding resources to declare.
REFERENCES
-
- Silk J. A new approach to the management of pretibial lacerations. Injury. 2001;32(5):373-376.
- Roybal LL, Howerter S, Markus B, et al. Use of a novel adhesive suture retention wound closure device to prevent patient follow-up visits during the COVID-19 pandemic. JAAD Case Reports. 2020;6(7):593-597.
- Farshchian M, Sklar LR. The pinch stitch: a pearl for suturing wounds under tension. J Drugs Dermatol. 2020;19(12):1262.
SOURCE
Otto, Tracey S., et al. “A Pearl for Pretibial and Forearm Repair Following Mohs Micrographic Surgery.” Journal of Drugs in Dermatology: JDD 23.5 (2024): 380-380.
Content and images published with permission from the Journal of Drugs in Dermatology.
Adapted from original article for length and style.
Did you enjoy this JDD Case Report? You can find more here.