
Calcipotriene is a synthetic Vitamin D3 analogue with various functions, including promoting cellular differentiation and reducing inflammatory cytokines. The unique mechanism of action of calcipotriene has expanded its utility beyond psoriasis to off-label uses for other dermatologic conditions. Calcipotriene is well tolerated and can be used in conjunction with other treatment modalities. We continue our series, “Therapeutic Cheat Sheet,” with a closer look at calcipotriene, which is FDA-approved for psoriasis.
Calcipotriene Therapeutic Cheat Sheet
Compiled by: Nidhi Shah, MD | Reviewed by: Adam Friedman, MD
TRADE NAME1-3
-
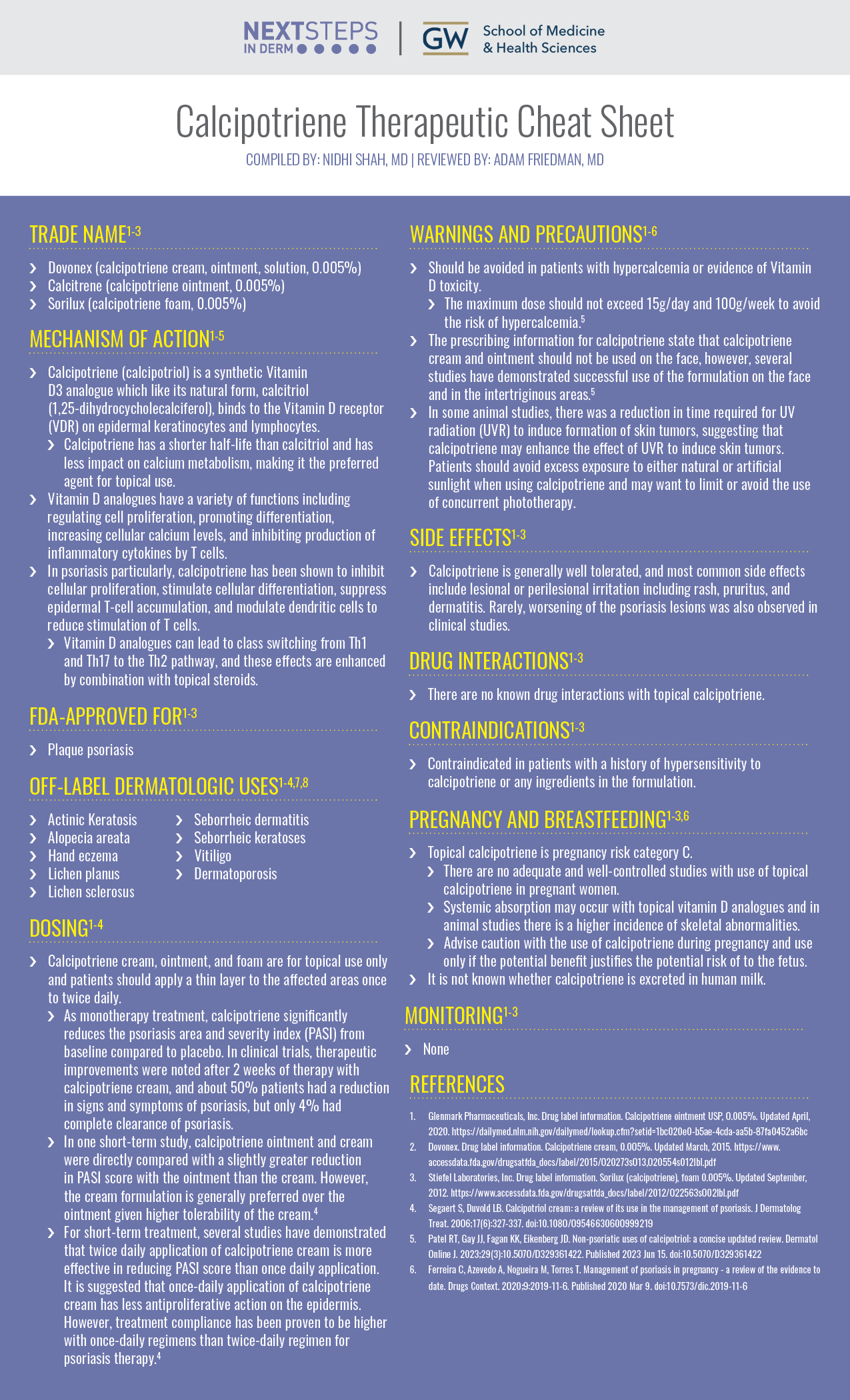
- Dovonex (calcipotriene cream, ointment, solution, 0.005%)
- Calcitrene (calcipotriene ointment, 0.005%)
- Sorilux (calcipotriene foam, 0.005%)
MECHANISM OF ACTION1-5
-
- Calcipotriene (calcipotriol) is a synthetic Vitamin D3 analogue which like its natural form, calcitriol (1,25-dihydrocycholecalciferol), binds to the Vitamin D receptor (VDR) on epidermal keratinocytes and lymphocytes.
- Calcipotriene has a shorter half-life than calcitriol and has less impact on calcium metabolism, making it the preferred agent for topical use.
- Vitamin D analogues have a variety of functions including regulating cell proliferation, promoting differentiation, increasing cellular calcium levels, and inhibiting production of inflammatory cytokines by T cells.
- In psoriasis particularly, calcipotriene has been shown to inhibit cellular proliferation, stimulate cellular differentiation, suppress epidermal T-cell accumulation, and modulate dendritic cells to reduce stimulation of T cells.
- Vitamin D analogues can lead to class switching from Th1 and Th17 to the Th2 pathway, and these effects are enhanced by combination with topical steroids.
- Calcipotriene (calcipotriol) is a synthetic Vitamin D3 analogue which like its natural form, calcitriol (1,25-dihydrocycholecalciferol), binds to the Vitamin D receptor (VDR) on epidermal keratinocytes and lymphocytes.
FDA APPROVED FOR1-3
-
- Plaque psoriasis
OFF-LABEL DERMATOLOGIC USES5
-
- Actinic Keratosis
- Alopecia areata
- Hand eczema
- Lichen planus
- Lichen sclerosus
- Seborrheic dermatitis
- Seborrheic keratoses
- Vitiligo
- Dermatoporosis
DOSING1-4
-
- Calcipotriene cream, ointment, and foam are for topical use only and patients should apply a thin layer to the affected areas once to twice daily.
- As monotherapy treatment, calcipotriene significantly reduces the psoriasis area and severity index (PASI) from baseline compared to placebo. In clinical trials, therapeutic improvements were noted after 2 weeks of therapy with calcipotriene cream, and about 50% patients had a reduction in signs and symptoms of psoriasis, but only 4% had complete clearance of psoriasis.
- In one short-term study, calcipotriene ointment and cream were directly compared with a slightly greater reduction in PASI score with the ointment than the cream. However, the cream formulation is generally preferred over the ointment given higher tolerability of the cream.4
- For short-term treatment, several studies have demonstrated that twice daily application of calcipotriene cream is more effective in reducing PASI score than once daily application. It is suggested that once-daily application of calcipotriene cream has less antiproliferative action on the epidermis. However, treatment compliance has been proven to be higher with once-daily regimens than twice-daily regimen for psoriasis therapy.4
- Calcipotriene cream, ointment, and foam are for topical use only and patients should apply a thin layer to the affected areas once to twice daily.
WARNINGS AND PRECAUTIONS1-6
-
- Should be avoided in patients with hypercalcemia or evidence of Vitamin D toxicity.
- The maximum dose should not exceed 15g/day and 100g/week to avoid the risk of hypercalcemia.5
- The prescribing information for calcipotriene state that calcipotriene cream and ointment should not be used on the face, however, several studies have demonstrated successful use of the formulation on the face and in the intertriginous areas.5
- In some animal studies, there was a reduction in time required for UV radiation (UVR) to induce formation of skin tumors, suggesting that calcipotriene may enhance the effect of UVR to induce skin tumors. Patients should avoid excess exposure to either natural or artificial sunlight when using calcipotriene and may want to limit or avoid the use of concurrent phototherapy.
- Should be avoided in patients with hypercalcemia or evidence of Vitamin D toxicity.
SIDE EFFECTS1-3
-
- Calcipotriene is generally well tolerated, and most common side effects include lesional or perilesional irritation including rash, pruritus, and dermatitis. Rarely, worsening of the psoriasis lesions was also observed in clinical studies.
DRUG INTERACTIONS1-3
-
- There are no known drug interactions with topical calcipotriene.
CONTRAINDICATIONS1-3
-
- Contraindicated in patients with a history of hypersensitivity to calcipotriene or any ingredients in the formulation.
PREGNANCY AND BREASTFEEDING1-3,6
-
- Topical calcipotriene is pregnancy risk category C.
- There are no adequate and well-controlled studies with use of topical calcipotriene in pregnant women.
- Systemic absorption may occur with topical vitamin D analogues and in animal studies there is a higher incidence of skeletal abnormalities.
- Advise caution with the use of calcipotriene during pregnancy and use only if the potential benefit justifies the potential risk of to the fetus.
- It is not known whether calcipotriene is excreted in human milk.
- Topical calcipotriene is pregnancy risk category C.
MONITORING1-3
-
- None
FURTHER READING
If you would like to learn more about calcipotriene, check out the following articles in the Journal of Drugs in Dermatology:
Preference for Cal/BDP Cream or Foam in Patients With Mild to Moderate Plaque Psoriasis
Kircik LH, Draelos ZD, Glick B, Green L, Burgess C
Abstract
Background: The combined use of topical calcipotriol/betamethasone dipropionate (Cal/BDP) is commonly used and demonstrated to be effective for the management of psoriasis and is shown to confer local anti-inflammatory and immunoregulatory effects. The use of the two agents in combination is synergistic. Despite the demonstrated efficacy of topically applied combination Cal/BDP, successful management of a chronic, relapsing inflammatory skin disease such as psoriasis in the real-world setting may be hindered if patients do not adhere to the dosing or frequency of application recommendations from their prescriber. Patient preference for and satisfaction with the topical treatment vehicle have been shown to influence adherence. A recent analysis has determined that patients perceived Cal/BDP cream vehicle with PAD technology as having favorable characteristics. This randomized, split-body study was undertaken to further assess patient satisfaction with Cal/BDP cream and Cal/BDP foam formulations.
Trial design: This was a split-body, subject-blind study. Study cream was administered in a single application to one side of the scalp and/or body; study foam was applied to the contralateral side. Patient self-administered questionnaires were completed before and after product application after a single site visit.
Results: Mean overall Vehicle Preference Measure (VPM) scores were higher for Cal/BDP cream than Cal/BDP foam (P=0.0043). Cal/BDP cream also achieved higher individual scores for ease of application, feeling to the touch, smell, and feeling on the skin (P<0.03). With regards to scalp application, subject assessments show that the cream was significantly more preferred in terms of limiting daily disruption (P=0.0008) Conclusion: Results of this study suggest that patients may prefer Cal/BDP cream over Cal/BDP foam for the management of psoriasis on the body and the scalp. Cal/BDP cream outperformed Cal/BDP foam on several specific measures of satisfaction and overall satisfaction measures.
J Drugs Dermatol. 2024;23(8):607-611.
Kontzias CL, Curcio A, Gorodokin B, et al.
Abstract
Background: Psoriasis affects diverse racial and ethnic groups. In July 2021, the US Food and Drug Administration approved calcipotriene/betamethasone dipropionate (CAL/BDP) 0.005%/0.065% cream to treat plaque psoriasis in adults. The efficacy and safety of CAL/BDP in patients with skin of color (SOC) who have psoriasis is not well characterized.
Method: A post hoc analysis of phase 3 clinical trial data (NCT03308799) was conducted to assess the efficacy, convenience, and safety of CAL/BDP cream versus CAL/BDP topical solution and vehicle cream in people with Fitzpatrick skin types IV to VI.
Results: This study included 784 participants, 280 (35.7%) of whom had Fitzpatrick skin types IV to VI. Patients treated with CAL/BDP cream had greater disease improvement, treatment convenience scores, and overall satisfaction than those treated with CAL/BDP topical solution in the subgroup with skin types IV to VI and the total study population. Adverse event rates were similar between the subgroup with skin types IV to VI and the total study population for all treatment arms.
Conclusion: Psoriasis is associated with a greater physical and psychosocial impact in patients with SOC. While many effective topical therapies exist, it may be helpful to conduct separate analyses of patients with SOC to assess the efficacy and safety of treatment in this population. This sub-analysis of phase 3 clinical trial data supports the efficacy and safety of CAL/BDP cream in the treatment of plaque psoriasis in patients with SOC. CAL/BDP cream also had greater convenience, formula acceptability, and overall satisfaction in both the subgroup with SOC and the total trial population, which may improve adherence to topical therapy and treatment outcomes for people with SOC who have psoriasis.
J Drugs Dermatol. 2023;22(7):668-672.
REFERENCES
-
- Glenmark Pharmaceuticals, Inc. Drug label information. Calcipotriene ointment USP, 0.005%. Updated April, 2020. https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=1bc020e0-b5ae-4cda-aa5b-87fa0452a6bc
- Drug label information. Calcipotriene cream, 0.005%. Updated March, 2015. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020273s013,020554s012lbl.pdf
- Stiefel Laboratories, Inc. Drug label information. Sorilux (calcipotriene), foam 0.005%. Updated September, 2012. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/022563s002lbl.pdf
- Segaert S, Duvold LB. Calcipotriol cream: a review of its use in the management of psoriasis. J Dermatolog Treat. 2006;17(6):327-337. doi:10.1080/09546630600999219
- Patel RT, Gay JJ, Fagan KK, Eikenberg JD. Non-psoriatic uses of calcipotriol: a concise updated review. Dermatol Online J. 2023;29(3):10.5070/D329361422. Published 2023 Jun 15. doi:10.5070/D329361422
- Ferreira C, Azevedo A, Nogueira M, Torres T. Management of psoriasis in pregnancy – a review of the evidence to date. Drugs Context. 2020;9:2019-11-6. Published 2020 Mar 9. doi:10.7573/dic.2019-11-6
Did you enjoy this Therapeutic Cheat Sheet? You can find more here.