
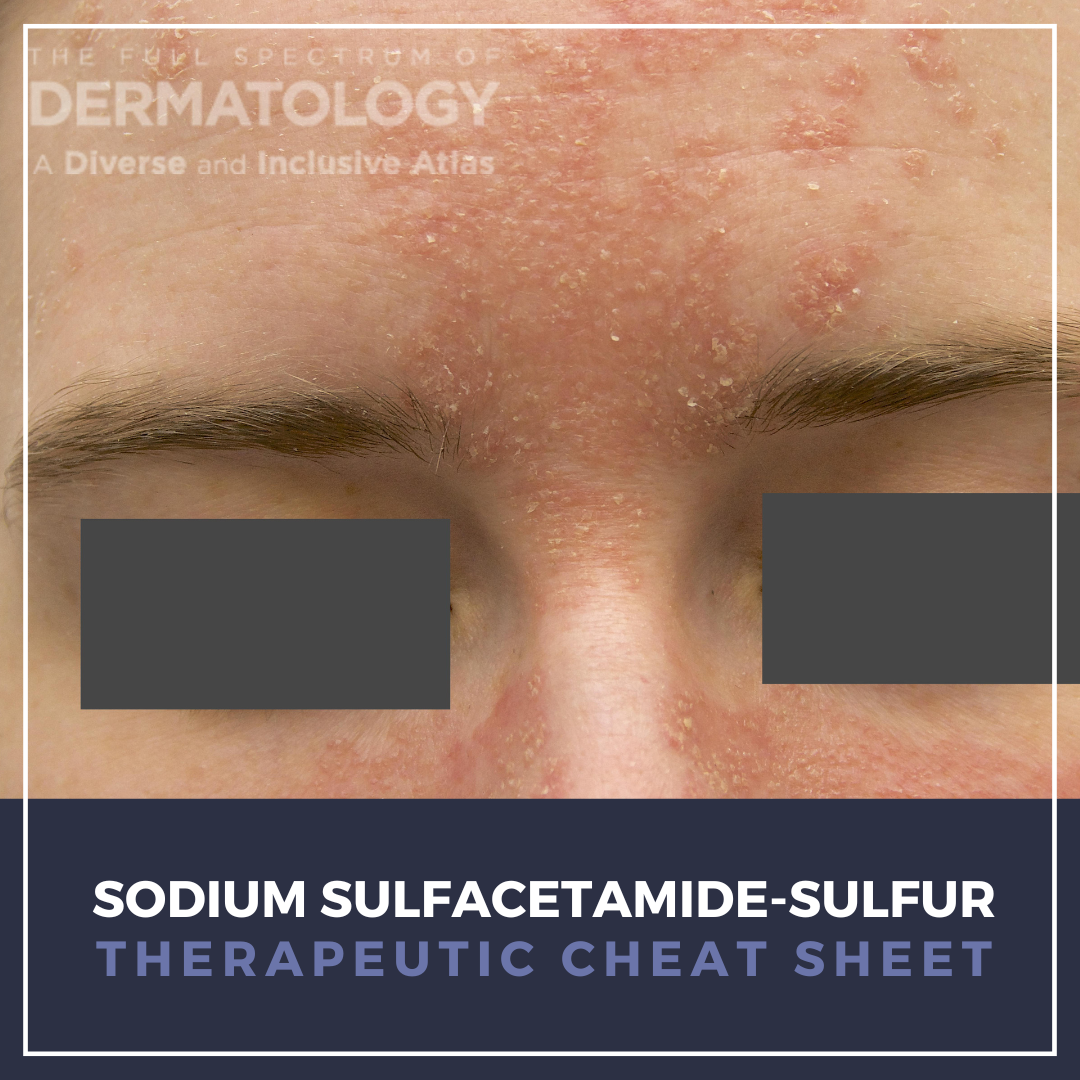
Sulfur–sulfacetamide is a long-standing topical therapy in dermatology valued for its combined antimicrobial, anti-inflammatory, and keratolytic effects. It is commonly used for several conditions including acne vulgaris, papulopustular rosacea, and seborrheic dermatitis. Although newer targeted therapies are often preferred for rosacea, sulfur–sulfacetamide remains a practical option, especially in patients with rosacea–seborrheic dermatitis overlap. In practice, its benefits should be balanced against tolerability as dryness and irritation are common side effects.
We continue our “Therapeutic Cheat Sheet” series with a focused review of sulfur–sulfacetamide’s dermatologic applications, safety considerations, and practical prescribing pearls.
Sodium Sulfacetamide-Sulfur Therapeutic Cheat Sheet
Compiled by: Robin Picavia, MD; Reviewed by: Adam J. Friedman, MD, FAAD
TRADE NAME
Plexion, Clenia, Rosanil, Rosac, Sulfacleanse
MECHANISM OF ACTION1,2
Sodium sulfacetamide is a sulfonamide antimicrobial agent that competitively inhibits para-aminobenzoic acid utilization, impairing bacterial folate synthesis and thereby limiting proliferation of susceptible cutaneous organisms, including Cutibacterium acnes. In addition to its antibacterial activity, sulfacetamide exhibits anti-inflammatory effects that contribute to clinical improvement in inflammatory acne and papulopustular rosacea. Sulfur provides complementary keratolytic and desquamative activity through interactions with keratin and sulfur-containing amino acids, facilitating stratum corneum shedding and reduction of follicular obstruction. The combination of sulfacetamide and sulfur has demonstrated efficacy in reducing inflammatory lesion counts and background erythema in rosacea, with utility in patients with overlapping seborrheic dermatitis phenotypes.
FDA-APPROVED INDICATIONS
Topical sulfur–sulfacetamide formulations are FDA approved for the treatment of acne vulgaris, rosacea (acne rosacea), and seborrheic dermatitis.
OFF-LABEL DERMATOLOGIC USES1,2,3,4
-
- Perioral (periorificial) dermatitis, particularly in mild or chronic cases where topical antibiotics or steroids are being avoided
- Pityriasis (tinea) versicolor, as a nonstandard option in mild cases when conventional antifungals are not tolerated or are ineffective
- Other inflammatory dermatoses with scale, where sulfur’s keratolytic properties are leveraged based on clinical experience rather than controlled trials.
DOSING1,3
• Leave-on formulations containing sulfacetamide 10% and sulfur 5% are typically applied once to three times daily, with many clinicians initiating once-daily use and titrating upward based on tolerability.
• Cleanser formulations are generally used once or twice daily, with avoidance of contact with the eyes, lips, and mucous membranes.
WARNINGS AND PRECAUTIONS1,5
• Sodium sulfacetamide carries class sulfonamide warnings, including rare but potentially serious hypersensitivity reactions such as agranulocytosis, hemolytic anemia, drug fever, and jaundice.
• Although systemic absorption is minimal with topical use, caution is advised in patients with known sulfonamide hypersensitivity, particularly when applied to inflamed or compromised skin.
• Local irritation, dryness, and erythema are common early in therapy and may necessitate dose reduction or discontinuation.
SIDE EFFECTS1,2
• Local cutaneous reactions including burning, stinging, erythema, scaling, and peeling are most common.
• Allergic contact dermatitis and hypersensitivity reactions are uncommon but reported.
• Severe systemic reactions are exceedingly rare but included in labeling due to sulfonamide class effects.
DRUG INTERACTIONS1
• Clinically significant systemic drug interactions are unlikely with topical therapy.
• Additive irritation may occur with concurrent use of retinoids, benzoyl peroxide, or alcohol-based topical agents.
CONTRAINDICATIONS1,2
• Known hypersensitivity to sulfonamides, sulfur, or any formulation component.
• Some product labels advise avoidance in patients with underlying renal disease.
PREGNANCY AND BREASTFEEDING
• Pregnancy category C under legacy FDA labeling; use only if potential benefit justifies potential risk.
• Data on topical use during lactation are limited; caution is advised due to known oral sulfonamide excretion in breast milk.
MONITORING
• Routine laboratory monitoring is not required.
• Clinical monitoring should focus on cutaneous tolerability and signs of hypersensitivity.
• Treatment response and adverse effects are typically reassessed after 6–12 weeks, consistent with clinical rosacea studies.
FURTHER READING
If you would like to read more about Sodium Sulfacetamide-Sulfur, check out the following articles in the Journal of Drugs in Dermatology:
Treatment of Papulopustular Rosacea with Sodium Sulfacetamide 10%/Sulfur 5%Emollient Foam
Trumbore, M. W., Goldstein, J. A., & Gurge, R. M. (2009). Treatment of papulopustular rosacea with sodium sulfacetamide 10%/sulfur 5% emollient foam. Cutis, 8(3), 299.
Abstract
Acne rosacea is a chronic cutaneous disorder affecting as many as 14 million Americans. Papulopustular rosacea is the classic form of rosacea characterized by papules, pustules, and erythema. The skin barrier deficiency and vascular hyperactivity characteristic of papulopustular rosacea increase skin dryness and irritation, which can be further exacerbated by medications commonly used to treat rosacea. Sodium sulfacetamide 10%/sulfur 5% emollient foam (SSSE foam) is formulated for topical administration and is fragrance free and alcohol free. This nonrandomized, noncontrolled, open-label, prospective case series was designed to evaluate the efficacy and safety of a SSSE foam for the treatment of papulopustular rosacea in 8 patients. Patients experienced clinically significant improvements in the severity of rosacea with a favorable safety profile, and reported of an improved quality of life. The high patient satisfaction ratings for SSSE foam suggest that the product may improve long-term compliance rates, with the potential to yield more favorable clinical outcomes.
Draelos, Z. D. (2010). The multifunctionality of 10% sodium sulfacetamide, 5% sulfur emollient foam in the treatment of inflammatory facial dermatoses. Cutis, 9(3), 234.
Abstract
Prior to 1962, some of the most versatile drugs in dermatology were approved by the U.S. Food and Drug Administration (FDA) solely on the basis of safety. One of these is the combination 10% sodium sulfacetamide and 5% sulfur. Sodium sulfacetamide possesses anti-inflammatory and antibacterial properties while sulfur is a nonspecific antibacterial and antifungal. A new emollient foam formulation of 10% sodium sulfacetamide and 5% sulfur allows a thinner application film and leaves behind no residue on hair bearing or nonhair bearing skin. The sulfur smell is also more quickly dissipated with reduced irritation. This uncontrolled, observational, prospective, open-label, single site, eight-week study enrolled 24 subjects (eight with rosacea, eight with seborrheic dermatitis, eight with acne vulgaris) to evaluate the safety and efficacy of this novel foam formulation. At eight weeks, statistically significant improvement was seen in inflammatory rosacea lesion counts and the signs of seborrheic dermatitis. A 50% reduction was noted in the total acne lesion counts. These findings confirm the versatility of an emollient 10% sodium sulfacetamide and 5% sulfur foam.
REFERENCES
-
- Trumbore MW, Goldstein JA, Gurge RM. Treatment of papulopustular rosacea with sodium sulfacetamide 10%/sulfur 5% emollient foam. J Drugs Dermatol. 2009 Mar;8(3):299-304. PMID: 19271381.
- Del Rosso JQ. The use of sodium sulfacetamide 10%-sulfur 5% emollient foam in the treatment of acne vulgaris. J Clin Aesthet Dermatol. 2009 Aug;2(8):26-9. PMID: 20729951; PMCID: PMC2923965.
- Torok HM, Webster G, Dunlap FE, Egan N, Jarratt M, Stewart D. Combination sodium sulfacetamide 10% and sulfur 5% cream with sunscreens versus metronidazole 0.75% cream for rosacea. Cutis. 2005 Jun;75(6):357-63. PMID: 16047874.
- Thiboutot D, Gollnick H, Bettoli V, Dréno B, Kang S, Leyden JJ, Shalita AR, Lozada VT, Berson D, Finlay A, Goh CL, Herane MI, Kaminsky A, Kubba R, Layton A, Miyachi Y, Perez M, Martin JP, Ramos-E-Silva M, See JA, Shear N, Wolf J Jr; Global Alliance to Improve Outcomes in Acne. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009 May;60(5 Suppl):S1-50. doi: 10.1016/j.jaad.2009.01.019. PMID: 19376456.
- Sharma A, Kroumpouzos G, Kassir M, Galadari H, Goren A, Grabbe S, Goldust M. Rosacea management: A comprehensive review. J Cosmet Dermatol. 2022 May;21(5):1895-1904. doi: 10.1111/jocd.14816. Epub 2022 Feb 14. PMID: 35104917.
- Del Rosso JQ. Evaluating the role of topical therapies in the management of rosacea: focus on combination sodium sulfacetamide and sulfur formulations. Cutis. 2004 Jan;73(1 Suppl):29-33. PMID: 14959943.
Did you enjoy this Therapeutic Cheat Sheet? You can find more here.