
At the 2026 ODAC Dermatology Conference in Orlando, Florida, Dr. Olayemi Sokumbi, MD delivered a masterclass on clinicopathologic correlation. A board-certified dermatologist and dermatopathologist widely recognized for her expertise in complex medical dermatology, Dr. Sokumbi showcased her special interest in diagnostic dilemmas in her talk. She emphasized the critical role of clinicopathologic correlation in resolving challenging cases, providing a powerful reminder to clinicians that the skin is a window to systemic disease.
Clinicopathologic Correlation
Dr. Sokumbi began the session with a charge to the audience: how can we better correlate clinicopathologic features to help improve diagnostic accuracy? Drawing from her experience, she emphasized that creating a structured way of thinking helps both clinicians and dermatopathologists to recognize specific reaction patterns. Once identified, these patterns can inform systemic associations. For example, an astute dermatopathologist can both establish a precise histopathologic diagnosis, but also communicate to clinicians when findings can signal underlying systemic disease, prompting clinicians to consider comprehensive evaluation if appropriate. Dr. Sokumbi reminded that multidisciplinary collaboration is essential to evaluate and treat systemic associations; this will lead to improved patient outcomes.
Case 1: Flesh-colored papules
Dr. Sokumbi utilized the power of storytelling to emphasize her take-home messages with two patient case examples. First, she described a patient vignette of a 51-year-old male with firm, flesh-colored papules along the helices of his bilateral ears who had previously received a diagnosis of skin tags. Over time he had noted increased development of papules and new involvement of the dorsal hands, along with symptoms of inflammatory arthritis.
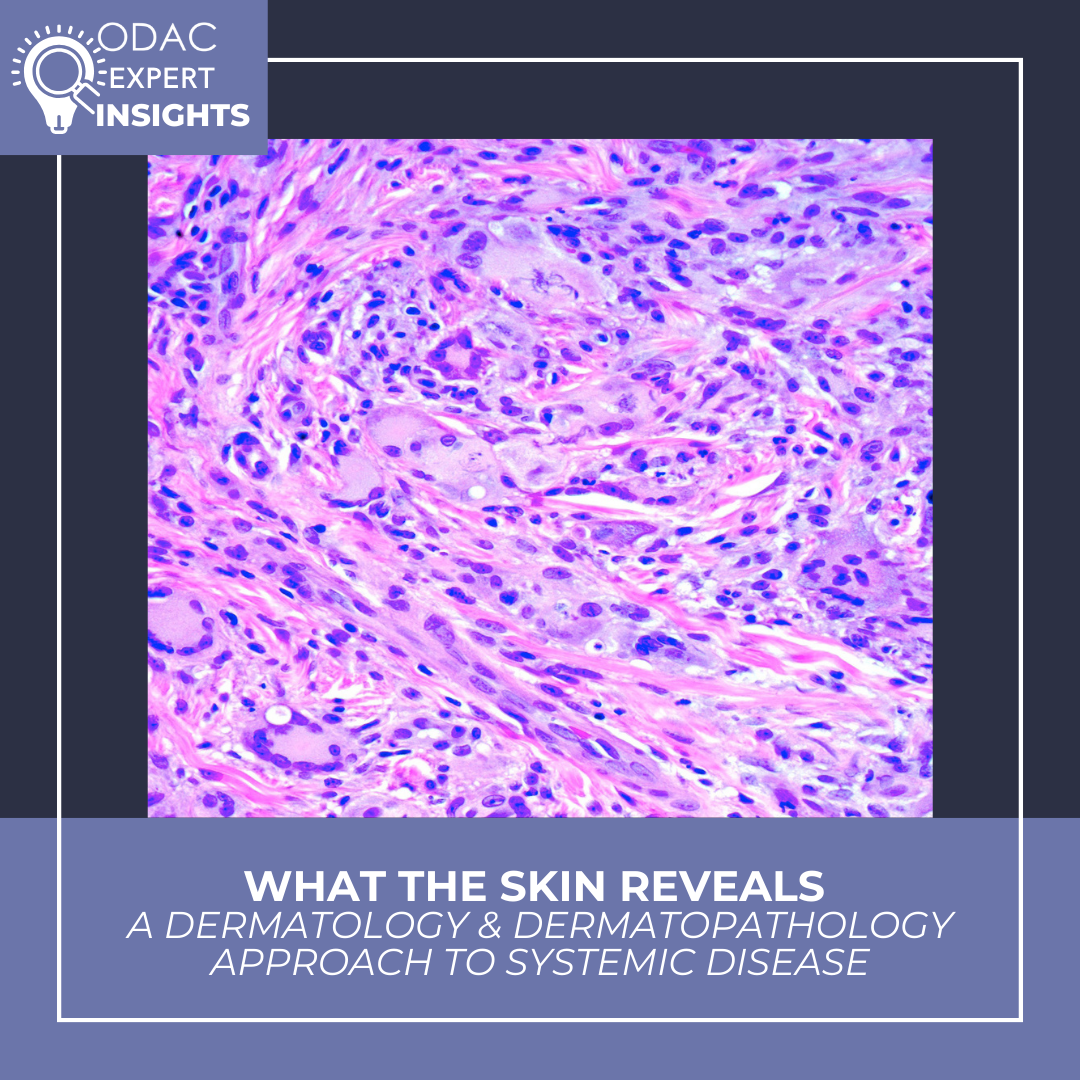
Biopsy of these lesions showed foamy, xanthomatized histiocytes in the dermis. Immunohistochemistry showed that cells were CD68 positive and CD1a negative. Applying the structured approach to pattern recognition, she first utilized an organized, recently revised, framework that divides histiocytoses and neoplasms of the macrophage-dendritic cell lineages into groups: Langerhans cell histiocytoses, cutaneous histiocytoses, Rosai-Dorfman Disease, malignant histiocytoses, and hemophagocytic lymphohistiocytoses. Working through the categories, she first noted that negative CD1a staining argues against Langerhans cell histiocytoses. She considered a rare diagnosis, Erdheim-Chester disease, a multisystem disorder of adulthood characterized by excess production and accumulation of histiocytes in affected tissues, however over 50% of cases are associated with somatic BRAF V600E mutation, and this patient’s testing was negative for this mutation, suggesting against this diagnosis. The case was not entirely clear when considering only the histopathologic findings.
Astutely, Dr. Sokumbi reminded that when the diagnosis is unclear, the answer is almost always at the bedside. Reflecting on the clinical morphology, she noted that the distribution of papules on the hands and periungual areas is clinically classic for multicentric reticulohistiocytosis. “Textbook” histology features of this condition include ground-glass cytoplasm, multinucleated giant cells, and dermal infiltrate of histiocytes, however, the disease can also present in non-classic ways and histologically mimic other lipidized histiocytoses. Here, clinicopathologic correlation was truly crucial for establishing the correct diagnosis of multicentric reticulohistiocytosis in this patient. Importantly, this condition is associated with severe destructive arthritis and has a significant association with malignancy, and has a starkly different treatment pathway from other mentioned conditions.
Case 2: Diffuse Skin Discoloration
The second clinical case detailed a female patient with diffuse skin discoloration, who was previously diagnosed with nonspecific hyperpigmentation but remained a diagnostic mystery. On exam, she was noted to have subtle diffuse discoloration of a majority of skin, especially prominent on the ears. Prior biopsies had shown mainly normal skin and had no obvious diagnostic features. Dr. Sokumbi’s structured differential included both internal and external causes of skin discoloration, such as argyria, lichen planus pigmentosus, and ochronosis. Upon closer inspection of this patient’s biopsy, Dr. Sokumbi noted some subtle pigment incontinence, but also abnormal elastic fibers, confirmed on an elastic tissue stain showing thickened and fragmented fibers. These findings clinched a diagnosis of ochronosis; however the patient had no relevant exogenous exposures. Upon workup, she was found instead to have alkaptonuria causing endogenous ochronosis. Alkaptonuria is an inborn error of metabolism caused by homogentisic acid oxidase deficiency which has characteristic skin findings along with systemic associations such as arthritis and cardiac involvement. Identifying this diagnosis is critical to prompt genetic and systemic evaluation.
Take-Home Messages
Dr. Sokumbi closed on poignant take-home messages that guide her when approaching complex cases and diagnostic dilemmas. First, clinicopathologic correlation is essential, but can occasionally require persistence and repeat biopsies. She encouraged that clinicians should not be afraid to re-biopsy if the story and the findings do not fit. Second, the skin can truly be a window into systemic disease: dermatologists and dermatopathologists may be the first to identify systemic conditions and should initiate multispecialty care when appropriate. The recognition of systemic associations can profoundly alter treatment decisions and patient outcomes.
This information was presented by Dr. Olayemi Sokumbi during the 2026 ODAC conference. The above highlights from her lecture were written and compiled by Dr. Erika McCormick. McCormick was one of the five residents selected to participate in the Young Dermatology Leader Mentorship Program sponsored by Sun Pharma and organized by Derm In-Review.