
CASE
A 47-year-old woman presented for Mohs Micrographic Surgery for a biopsy-proven basal cell carcinoma involving the right nasal ala. The patient had a history of basal cell nevus syndrome (BCNS) and previous history of multiple basal cell carcinomas.
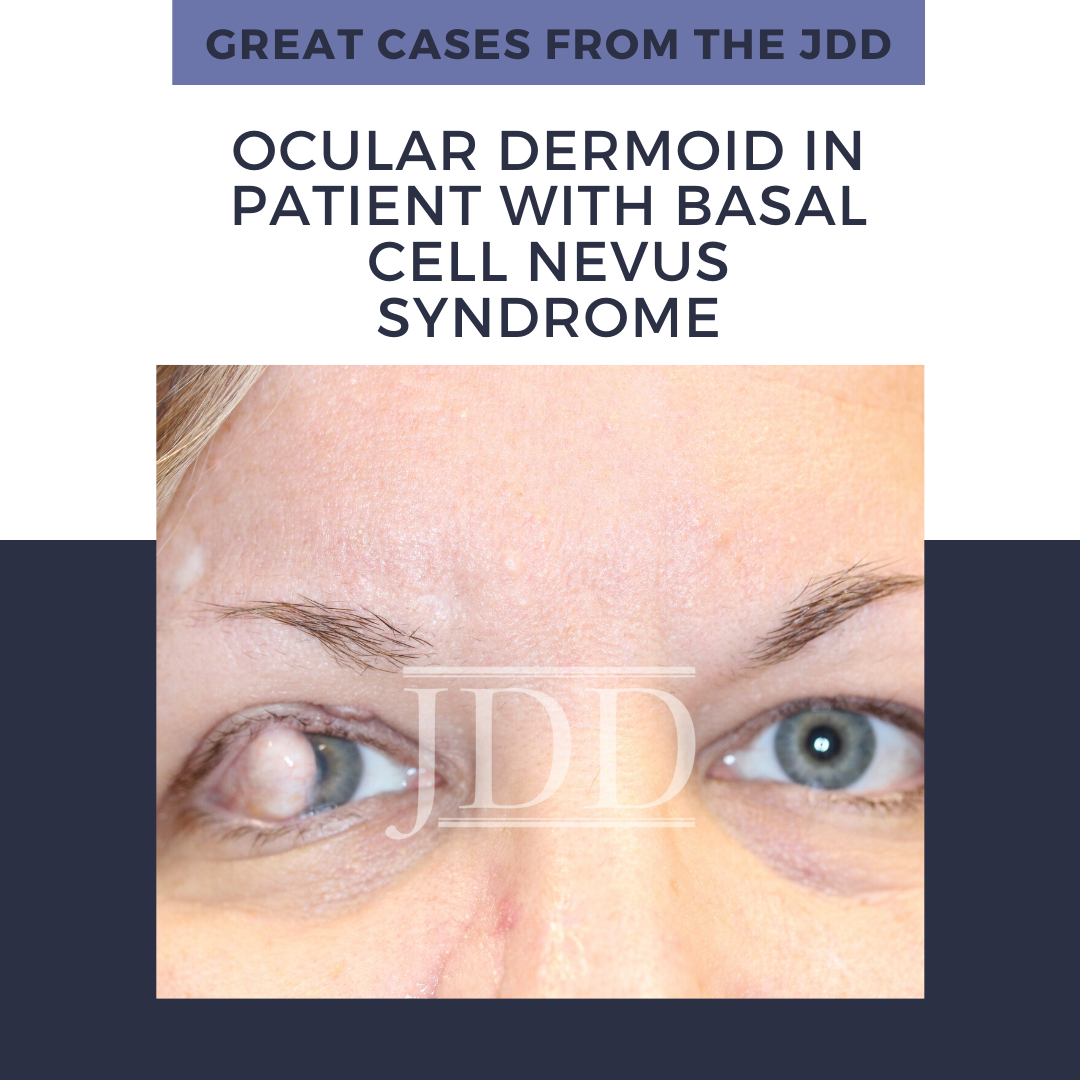
On initial examination, the patient was noted to have a few scattered pearly molluscoid papules on the head and neck, which were suspicious for early basal cell carcinomas. The patient was also noted to have a 1 cm dome-shaped nodule on the lateral corneal-scleral junction of the right upper eyelid (Figures 1 and 2). On palpation, the lesion was firm and rubbery but was not fluctuant. The patient was a poor historian, however, on further questioning, the patient noted decreased visual acuity in the right eye and stated that she had had the lesion for many years. She had last seen an ophthalmologist over 20 years ago and was unsure if she had the eyelid lesion at that time. There was no lymphadenopathy on exam and the patient stated that she otherwise felt well.

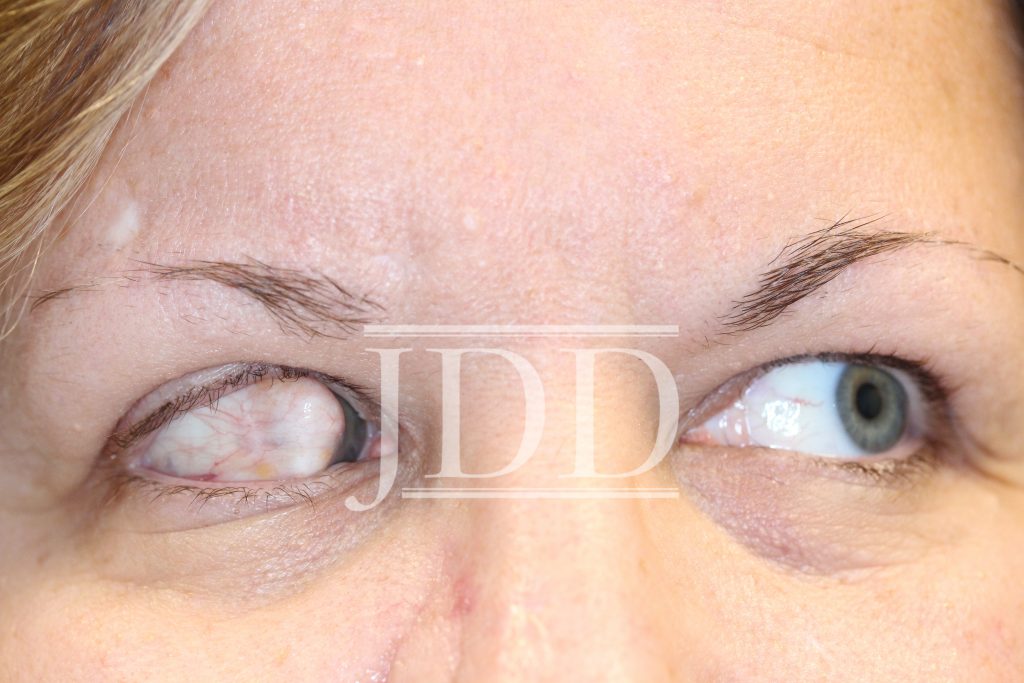
On obtaining previous records, it was discovered that the patient had the lesion at least since the age of one year. The lesion was biopsied by a pediatric ophthalmologist and found to be an ocular dermoid. No further treatment was recommended at that time as the lesion was not obstructing vision. The lesion subsequently grew and began to obstruct vision; however, no surgical treatment was performed.
Ocular dermoids are uncommon tumors, which are rarely seen by dermatologists. They represent the misplacement of dermal tissues and are frequently associated with cutaneous auricular appendages and first branchial arch anomalies.1 The most commonly associated auricular appendages are accessory tragi and preauricular sinuses.2 Definitive treatment of dermoids can be achieved by surgical resection, however, determining which lesions should be surgically removed is a topic of debate. A case series published in 2015 recommended that all dermoids affecting the visual axis, dome shaped, or causing conjunctival injection/irritation, be surgically removed.3 Additionally, patients who were undergoing removal of auricular appendages or had parents who desired cosmetic removal, could also be considered for removal. Due to the risk of general anesthesia, every effort should be made to schedule removal concurrently with any other necessary surgeries.3
Although a rarely encountered entity by dermatologists, they should be aware of this condition and its associated management. Delay in treatment can lead to significant lifelong impairment of visual acuity. Additionally, ocular dermoids are commonly associated with preauricular sinuses and accessory tragi. Therefore, patients presenting to dermatology with preauricular sinuses or accessory tragi should be considered for ocular exam. Interestingly, our patient also had a history of BCNS. Based on the authors’ review of the literature, there are no published reports of ocular dermoid tumors in association with BCNS, however, there is one report of a midline nasal dermoid cyst in association with BCNS.4 Larger population-based studies or additional case reports should be reported to better assess any possible link between BCNS and dermoid cysts. 9
References
Source:
Mihir Shah MD, William Hanke MD MPH (2020). Ocular Dermoid in Patient With Basal Cell Nevus Syndrome, 19 (7). https://jddonline.com/articles/dermatology/S1545961620P0792X
Content and images used with permission from the Journal of Drugs in Dermatology.
Adapted from original article for length and style.
Did you enjoy this case report? Find more here.