

At the 16th Annual ODAC Dermatology, Aesthetics and Surgical Conference held January 18th-21st, 2019 in Orlando, FL, longtime meeting Vice Chair Dr. Joel L. Cohen from Denver Colorado, spoke on perioral combination therapy. His presentation outlined his approach to perioral rejuvenation with one main theme – combination treatment, combination treatment, combination treatment. Simply put, combination treatment for perioral rejuvenation yields the most optimal results.
Dr. Cohen’s Approach
Dr. Cohen’s approach to perioral rejuvenation begins by dividing his work into its requisite parts. If the patient has excessive animation, toxins are recommended. If the patient has only a few superficial etched lines, fillers are recommended. If the patient has more significant or many perioral rhytides, laser resurfacing is the tool of choice – but he emphasizes full-field erbium over fractional options for significant etched-lines (see figure 1). Overall, all three should be considered individually or in combination to yield the best results. A major take home point regarding perioral rhytides is that fillers and toxins are not the primary treatment for this condition — and patients with etched-lines on the upper lip really need laser resurfacing.

His presentation also highlighted the need to address the entire perioral area when treating cutaneous lip etching – such as fillers in the nasolabial folds, antero-medial cheek, secondary smile lines, marionette area, and pre-jowl sulcus.
When addressing the mucosal lips as far as lip volume, it is of the utmost importance to make sure patients have a realistic expectation of results. Dr. Cohen prefers to use the Merz lip fullness scale, one of the scales that he co-authored. With this scale, no patient should jump from a zero to a four. Patients should move one or two grades on the scale in order to keep the result looking natural – and to be honest, it often isn’t even realistic for someone with really skinny lips to augment to full grade 4 lips, the anatomy just doesn’t accommodate that type of change.
It’s also important to note that mucosal lip-augmentation often results in neo-collagenesis over time. Therefore, it is important to get volume and proportions right in the first place, and not just simply squirt a lot of volume all over the lip or even uniformly throughout the lip. The medial lip should be fuller than the lateral lip. And the lip should have tubercles of projection points.
When treating the orbicularis oris muscle with toxin, Dr. Cohen recommends 5-10 units of botulinum toxin total (Botox, Xeomin units) or 12-20 units of Dysport. He notes that more is not better in perioral area, because in a clinical trial that he did with Botox into the perioral lip columns visible at animation (J Cohen, S Dayan, S Cox. Dermatologic Surgery), duration doesn’t seem to be significantly longer but yet higher doses can be associated with more adverse events as far as muscular oral competence.
When treating moderate to severe etched-in cutaneous upper and lower lip rhytides, he prefers full-field erbium resurfacing – he sees it as “picking the right tool for the job”. He often likes to try to treat the upper and lower cutaneous lip orbicularis oris prominence with botulinum toxin a week or two prior to the resurfacing. This is done to not only attempt some post-laser “chemo-immobilization” and try to avoid muscle contraction simply imprinting lines in exactly the spots that were present prior to the laser resurfacing, but also some recent studies have shown a more favorable cytokine and chemokine profile during the wound-healing response.
Setting Expectations for Healing
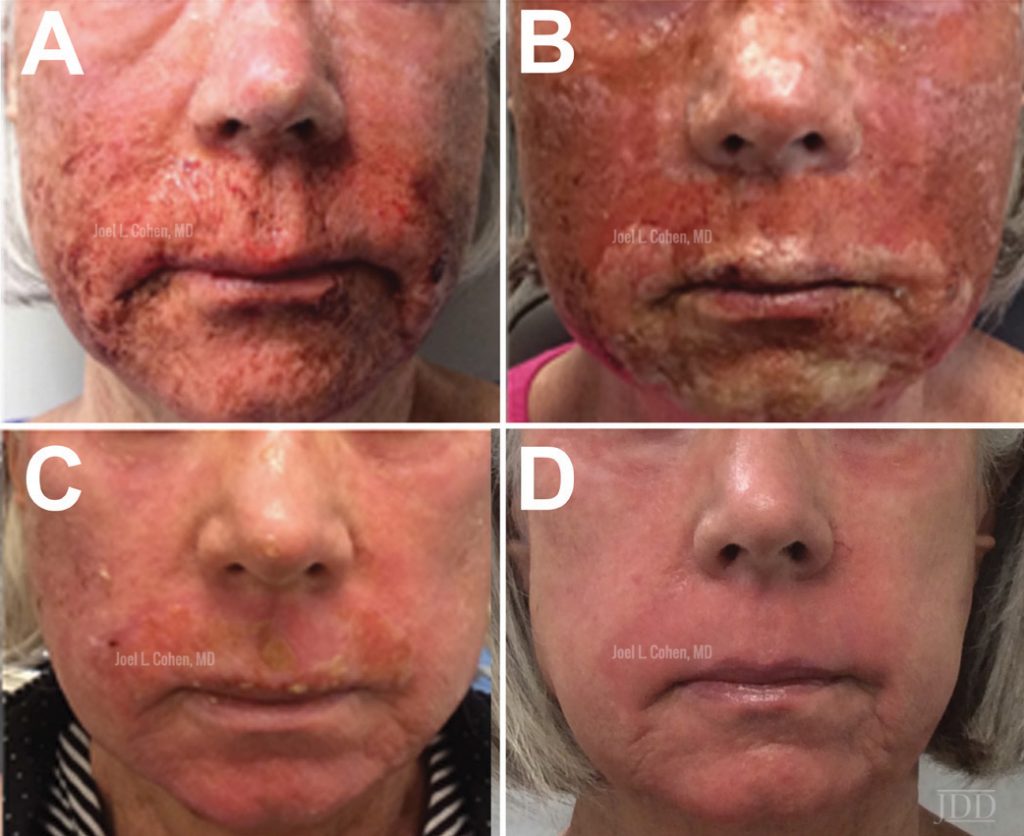
Dr. Cohen also stressed the importance of setting expectations for healing and results prior to treatment. Yellow and crusted healing around mouth is expected after full-field erbium resurfacing-(see figure 2), and this fibrin looks different than infection. Patients will also be red for some period of time after the full-field erbim treatment – sometimes a few weeks, and sometimes even a couple of months. For this reason, he explains that it’s a good idea to show patients pictures of what they can expect. And in terms of work flow, it is most helpful to have separate waiting rooms or at least schedule these patients for post-laser follow-up in the days following the treatment at a certain time of day less visible to other patients in your clinic (because they will look scary for other patients). He advises against doing BTX-A on the same day, however, as lasers (and even some peels) could cause swelling and swelling may, in turn, cause migration of toxin.
Other Considerations
In addition, BTX-A can be helpful to pretreat anticipated areas of large Mohs repairs, especially in high tension areas. The forehead, glabella, and crow’s feet are good anatomic locations for this treatment before Mohs or before repair of larger skin cancer defects on the face. (Flynn, Timothy. Dermatologic Surgery).
Of important note, physicians who do cosmetic work should really try to take good quality photos at baseline and in the weeks and several months post-resurfacing. Patients can forget how they looked before a procedure, and the full effect of the resurfacing can take 3-4 months in many cases. In this intervening time before follow-up appointments, sun-protection is absolutely key.
(A)

(B)
This information was presented by Dr. Joel L. Cohen at the 16th Annual ODAC Dermatology, Aesthetics and Surgical Conference held January 18th-21st, 2019 in Orlando, FL.
All images represent work done by Dr. Joel L. Cohen (Denver, CO) and have been copyrighted and published in the Journal of Drugs in Dermatology.
Figure 1 https://jddonline.com/articles/dermatology/S1545961615P1363X/2
Figure 2 https://jddonline.com/articles/dermatology/S1545961618P0796X/2
Figure 3 https://jddonline.com/articles/dermatology/S1545961616P0111X/2
Did you enjoy this post? Find more on Aesthetic Derm topics here.