Learn more about what it’s like to be a dermatologist today and what it takes to transition from residency to being a practicing dermatologist.
Find hands-on clinical pearls to help you care for your patients more effectively, stay up-to-date with the latest research, or stop by often for expert advice from industry leaders and insights on what it takes to be a key opinion leader.
Reflectance Confocal Microscopy (RCM) is a new noninvasive skin imaging modality that is comparable to traditional histopathology. Authors Radhika Srivastava BA, Catherine Reilly BS, Gina Francisco MBS, Hamza Bhatti DO, and Babar K. Rao MD present serial in vivo RCM imaging of an atypical nevus after shave excision over a 1-month period. Findings on RCM images are consistent with the inflammatory, proliferative, and remodeling phases of wound healing, and RCM may serve as a new tool to study wound healing in vivo over time.
Background
Reflectance Confocal Microscopy (RCM) is a new tool in the diagnosis and monitoring of skin disease. RCM uses an 830 nm laser to illuminate the skin and captures horizontal cross-sectional 8 mm X 8 mm mosaic images with high resolution. RCM has been used in the diagnosis of skin cancer and inflammatory skin diseases with good sensitivity and specificity,1,2 but the use of RCM to study wound healing is recently being explored. Traditionally, animal models have been used to study wound healing. Wound healing research in humans can pose several challenges, including difficulty in obtaining biopsy at the same location multiple times, and iatrogenic changes induced in the skin due to the act of performing biopsies. In comparison, the in vivo non-invasive nature of RCM allows clinicians to capture images of skin over time without patient discomfort due to repeated biopsies. RCM has been used to study wound healing after laser treatment, cryosurgery, burn wounds, and chronic wounds,3,6 but to our knowledge, it has never been used to describe wound healing after an acute surgical wound such as a shave excision. We present serial in vivo reflectance confocal microscopy characteristics of wound healing after shave excision of an atypical nevus over a 1-month period and discuss the role of RCM in monitoring wound healing over time.
Materials and Methods
A patient presented to our clinic with a suspicious pigmented nevus approximately 2.5 mm X 6 mm in size that was described as “changing and growing” over the course of 3 months. This lesion was visualized under dermoscopy and RCM (Vivascope 1500, Caliber ID, Rochester, NY). On RCM, it was noted that this melanocytic nevus had moderate cellular atypia, therefore the decision was made to perform a shave excision. Serial images of the wound were taken using RCM before shave excision and at days 1, 7, 21, and 28 days after removal. Horizontal mosaic images were acquired and analyzed by an expert confocal reader. A timeline of epithelialization, cellular infiltrate, and connective tissue deposition was reported in conjunction with prevailing observations.
Results
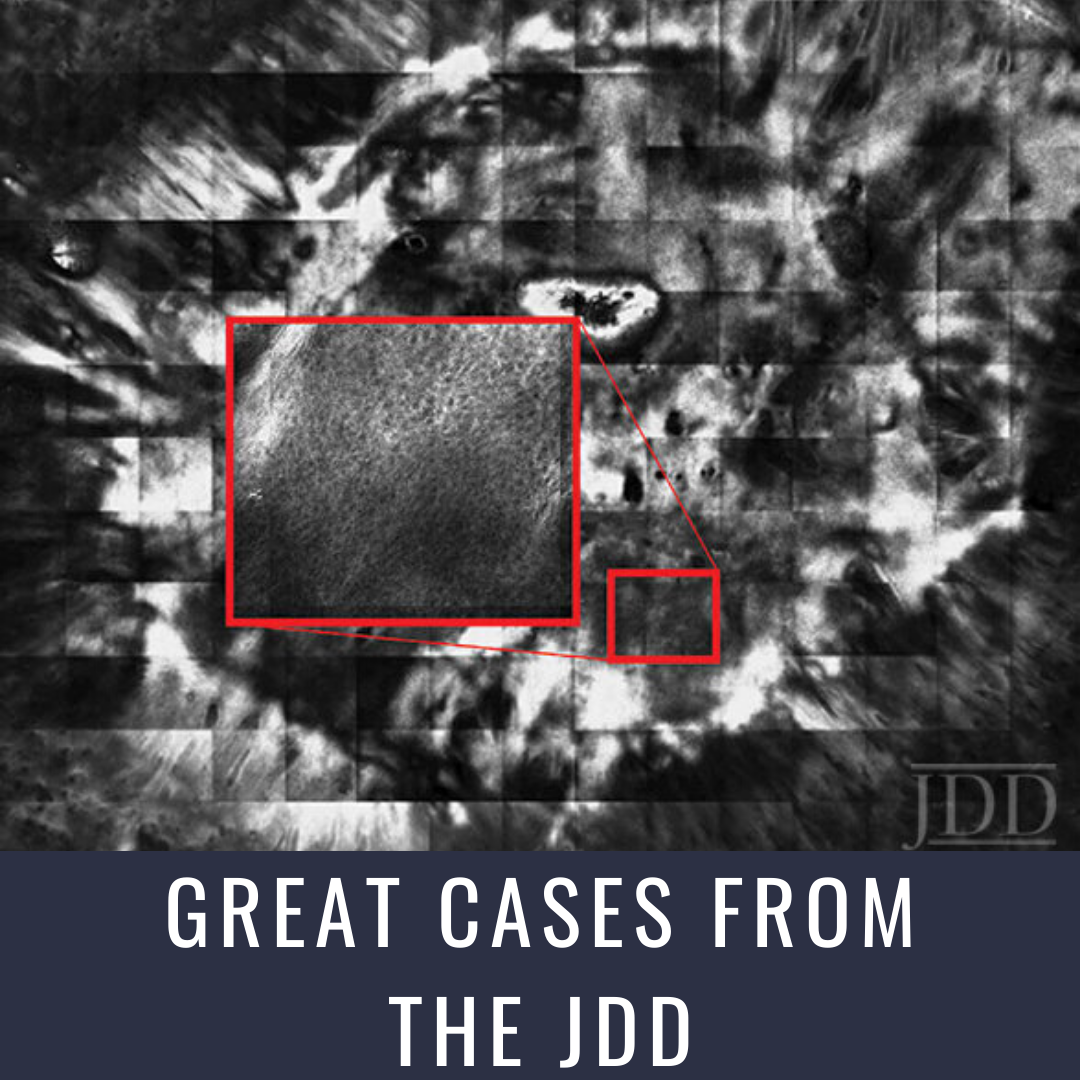
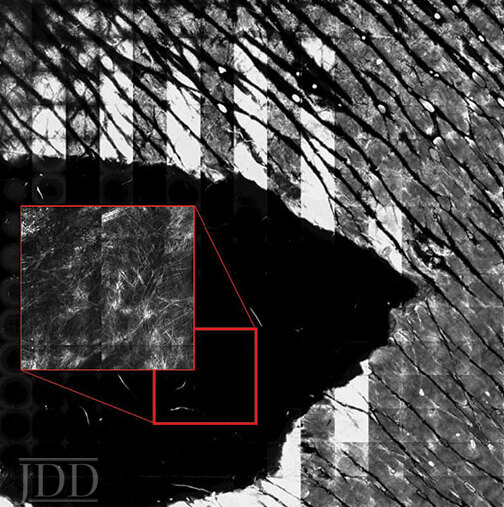
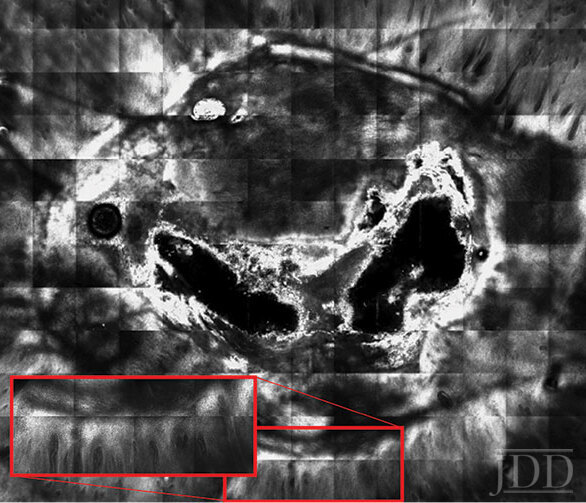
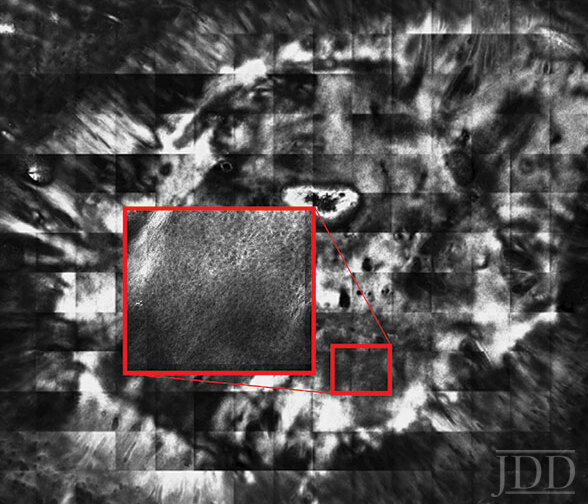
RCM of the wound on day 1 after removal shows a large black ovoid defect, as well as numerous small bright cells and linear fibrillary structures in the middle of the wound corresponding to the acute inflammatory phase of wound healing (Figure 1). RCM of the wound on day 7 shows an ovoid black defect in the skin surrounded by normal honeycomb pattern. Numerous bright cells and an irregular honeycomb pattern with focal polarization are present at the edges (Figure 2). RCM of the wound on day 21 shows a symmetrical ovoid area surrounded by an irregular honeycomb pattern. The dark circular defect has decreased in size, representing wound healing and re-epithelialization of the wound. The irregular honeycomb pattern of newly formed epidermis contains focal chronic inflammatory cells. Numerous dilated vessels are present, indicating the proliferative phase of wound healing (Figure 3). RCM of the wound on day 28 shows a well demarcated ovoid area with regular honeycomb pattern and minimal small bright cells, corresponding to resolving inflammation and the remodeling phase of wound healing (Figure 4).
Figure 1. The larger image is of the epidermis and shows a large black ovoid defect. The insert shows small bright cells and linear, fibrillary structures in the center of the wound.Figure 2. The larger image is of the epidermis and shows the black ovoid defect. The insert is also of the epidermis and shows small bright cells at the edges of the defect.
Figure 3. The lager image is of the epidermis and shows reepithelialization and subsequent decrease in size of the defect. The insert is of the dermis and shows multiple dilated blood vessels.Figure 4. The larger image is of the epidermis and shows reepithelialized wound. The insert is also of epidermis and shows regular honeycomb pattern of the newly formed epidermis from the center of the wound.
Discussion
The RCM images on day 1 show small bright cells and fibrillary structures that may correspond to neutrophils and exudate of the inflammatory phase. The RCM images on day 7 and 21 show an irregular honeycomb pattern and decrease in defect size, corresponding to re-epithelialization. The RCM image on day 21 shows multiple dilated vessels, corresponding to new vessel growth of the proliferative phase of wound healing. The RCM image on day 28 shows a regular honeycomb pattern and minimal small bright cells corresponding to resolving inflammation and the tissue remodeling phase of wound healing. RCM imaging shows that the inflammatory phase occurs within 1-7 days after insult, the proliferative or new tissue formation phase occurs within 1-4 weeks, and the remodeling phase occurs from 4 weeks to months or years, which is consistent with the physiology of wound healing.7 RCM has several benefits as compared to biopsy and histopathology in the study of wound healing. RCM allows the same location of the skin to be imaged over time. Additionally, the patient is able to avoid the discomfort of multiple biopsies, and clinicians are able to study the skin morphology without any iatrogenic disruption secondary to biopsy.A technical limitation of our methodology is poor contact of the scope secondary to the depressed nature of the wound bed. A new reflectance confocal microscope model has a handheld microscope head (Vivascope 3000, Caliber ID, Rochester, NY) that is significant smaller than the model used in this paper and captures 750 μm X 750 μm horizontal images. Manual pressure exerted on this handheld microscope allows improved contact with the varying topography of skin, but it can be difficult to correlate individual images produced with the location of the lesion. Complex algorithms utilizing the handheld microscope are being developed to stich individual images together and correlate the image taken with the clinical location, but such programs are not yet widely available.8 The traditional RCM model was selected to image this wound due to its ability to visualize the entire lesion and surrounding tissue in one 8 mm X 8 mm mosaic image, maintaining the geography of findings relative to the lesion, rather than multiple smaller images that would have been produced by the handheld microscope. Future studies are needed to optimize RCM methodology to monitor wound healing.
Conclusion
This case documents serial in vivo RCM imaging of a wound following shave excision, and our findings are consistent with what is known about the stages of wound healing.
References
Rajadhyaksha M, Marghoob A, Rossi A, Halpern AC, Nehal KS. Reflectance Confocal Microscopy of Skin In Vivo: From Bench to Bedside. Lasers Surg Med. 2017; 49(1):7–19.
Rao BK, John AM, Francisco G, Haroon A. Diagnostic Accuracy of Reflectance Confocal Microscopy Skin. Arch Pathol Lab Med. 2018 Oct 8.
Cameli N, Mariano M, Serio M, Ardigò M. Preliminary comparison of fractional laser with fractional laser plus radiofrequency for the treatment of acne scars and photoaging. Dermatol Surg. 2014; 40(5):553-61.
Stumpp OF, Bedi VP, Wyatt D, Lac D, et al. In vivo confocal imaging of epidermal cell migration and dermal changes post nonablative fractional resurfacing: study of the wound healing process with corroborated histopathologic evidence. J Biomed Opt. 2009;14(2):024018.
Terhorst D, Maltusch A, Stockfleth E, Lange-Asschenfeldt S, et al. Reflectance confocal microscopy for the evaluation of acute epidermal wound healing. Wound Repair Regen. 2011;19(6):671-9.
Lange-Asschenfeldt S, Bob A, Terhorst D, Ulrich M, et al. Applicability of confocal laser scanning microscopy for evaluation and monitoring of cutaneous wound healing. J Biomed Opt. 2012;17(7):076016.
Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature. 2008;453(7193):314-21.
Kose K, et al. Automated video-mosaicking approach for confocal microscopic imaging in vivo: an approach to address challenges in imaging living tissue and extend field of view. Sci Rep. 2017;7(1):10759. doi: 10.1038/s41598-017- 11072-9
Source:
R. Srivastava BA,C. Reilly BS,G. Francisco MBS,H. Bhatti DO, B. K. Rao MD, (2019). Life of a Wound: Serial Documentation of Wound Healing After Shave Removal Using Reflectance Confocal Microscopy. Journal of Drugs in Dermatology,18(5), 472-474. https://jddonline.com/articles/dermatology/S1545961619P0472X/3/