
Antihistamines, particularly second-generation histamine H1-receptor antagonists, are widely used in dermatology due to their antihistaminic activity and favorable safety profile characterized by minimal sedation compared with first-generation agents. They primarily act as peripheral H1-receptor antagonists, reducing histamine-mediated effects such as vasodilation, increased vascular permeability, and sensory nerve stimulation. Compared to first-generation antihistamines, second-generation agents demonstrate minimal penetration of the blood-brain barrier, resulting in a lower risk of sedation and improved tolerability for long-term use. Several second-generation H1-antihistamines are commonly prescribed, including cetirizine, loratadine, fexofenadine, levocetirizine, and desloratadine.
We continue our series, “Therapeutic Cheat Sheet,” with a closer look at the dermatologic applications of cetirizine and loratadine, two of the most commonly used second-generation H1-antihistamines in dermatology. They are FDA-approved for the treatment of allergic rhinitis and chronic spontaneous urticaria.
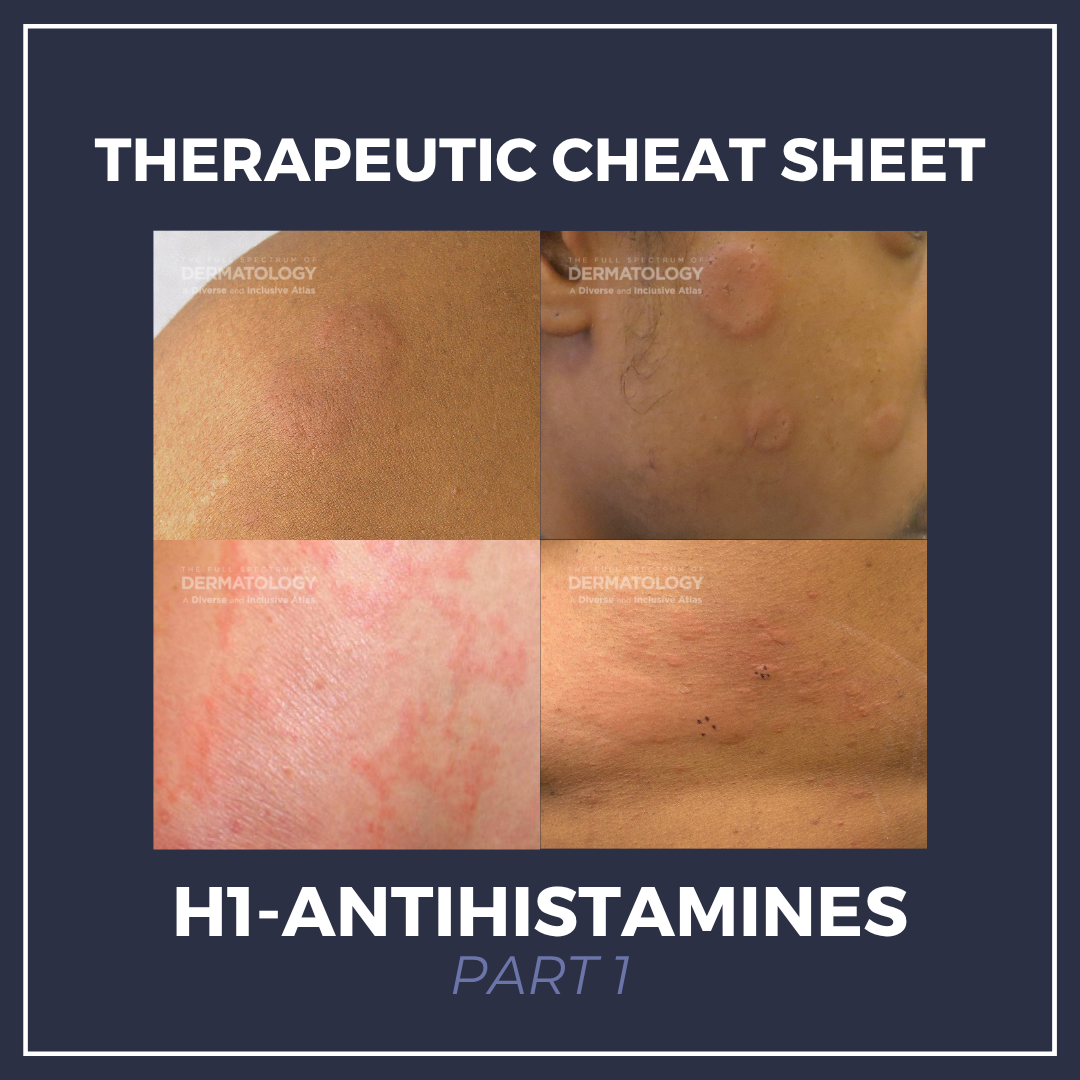
H1-Antihistamines Therapeutic Cheat Sheet (Part 1)
Compiled by: Nathaniel Lampley, MD | Reviewed by: Adam Friedman, MD
TRADE NAME
-
- Cetirizine: Zyrtec®1
- Loratadine: Claritin®2
MECHANISM OF ACTION1,3,4
-
- Predominantly act as peripheral histamine H1-receptor antagonists that inhibit histamine-mediated responses including vasodilation, increased vascular permeability, and sensory nerve stimulation.
- Minimal central nervous system penetration due to low blood-brain barrier permeability, resulting in lower risk of sedation compared to first generation H1-antihistamines.
FDA-APPROVED FOR1,2,3
-
- Seasonal Allergic Rhinitis: relief of symptoms associated with seasonal allergic rhinitis in adults and children 2 years of age and older.
- Perennial Allergic Rhinitis: relief of symptoms associated with perennial allergic rhinitis in adults and children 6 months of age and older (≥2 years for loratadine)
- Chronic Urticaria: treatment of the uncomplicated skin manifestations of chronic spontaneous urticaria in adults and children 6 months of age and older (≥2 years for loratadine)
OFF-LABEL DERMATOLOGIC USES
-
- Mast Cell Activation Disorder5
- Psoriasis6
- Lichen Planopilaris7
- Erythromelalgia8
- Eosinophilic Cellulitis9
- Eosinophilic Pustular Folliculitis8
- Vesiculobullous Darier Disease10
- Atopic Dermatitis11
- Alopecia Areata8
- Androgenic Alopecia12
- Eosinophilic Fasciitis8
DOSING1, 2, 3, 13
-
- Cetirizine:
- Adults and children ≥6 years: 5-10 mg once daily
- Children 6 months-5 years: 2.5 mg once daily (may increase to 5 mg/day in select patients)
- Loratadine:
- Adults and children ≥6 years: 10 mg once daily
- Children 2-5 years: 5 mg once daily
- Dose adjustment: Recommended in patients with renal and/or hepatic impairment
- Up-dosing (guideline-supported, off label): In patients with chronic urticaria who remain symptomatic, second generation H1 antihistamines may be up-titrated up to 4 times the standard daily dose under practitioner supervision.
- Cetirizine:
WARNINGS AND PRECAUTIONS1, 3, 4
-
- Somnolence may occur; caution with driving or operating potentially dangerous machinery
- Concomitant use with alcohol or CNS depressants should be avoided as this may cause additional reduction in alertness or CNS performance.
- Patients with hepatic and/or renal impairment should use caution.
- Use caution in elderly patients due to possible decreased renal function.
SIDE EFFECTS 1, 2, 3
-
- Primary side effects include somnolence, fatigue, dry mouth, dizziness, headache, and pharyngitis. Somnolence appears to be a dose-dependent effect and less common in loratadine.
- Uncommon side effects include abdominal pain, pharyngitis, cough, nausea, hypersensitivity reactions, hepatic transaminase elevation, severe hypotension, anaphylaxis, hemolytic anemia, thrombocytopenia, orofacial dyskinesia, cholestasis, glomerulonephritis, hepatitis, agitation, and insomnia.
DRUG INTERACTIONS1, 3, 4
-
- CNS depressants: concurrent use with CNS depressants may increase the risk of sedation.
- Pitolisant: concurrent use may reduce therapeutic efficacy of pitolisant (pharmacodynamic antagonism at histamine pathways).
- Cetirizine:
- P-glycoprotein interactions (e.g., verapamil, erdafitinib): concurrent cetirizine use may alter cetirizine CNS exposure and increase antihistaminic effects.
- Loratadine:
- CYP450-mediated interactions: Loratadine is primarily metabolized by CYP3A4 and CYP2D6; CYP3A4 inhibitors may increase loratadine plasma concentrations
CONTRAINDICATIONS1,2
-
- Absolute contraindications include patients with a known hypersensitivity to the agent or any of its ingredients.
PREGNANCY AND BREASTFEEDING
-
- Pregnancy: Classified as a former FDA Pregnancy Category B (animal studies negative; no clear human risk), however the American College of Obstetricians and Gynecologists and the American College of Allergy, Asthma, and Immunology (ACOG-ACAAI) recommends as an acceptable option for pregnant patients who require antihistamine therapy; however, it should be used during pregnancy only when necessary.3
- Breastfeeding: Generally considered compatible with breastfeeding at standard doses. However, prolonged use or higher doses may increase the risk of infant drowsiness.3,4
FURTHER READING
If you would like to learn more about antihistamines in dermatology, check out the following articles in the Journal of Drugs in Dermatology:
Vesiculobullous Darier Disease Symptomatically Responsive to Cetirizine
J.Wang, M. Lederhandler, N. Brinster, N. Soter MD
ABSTRACT
Darier disease is an autosomal dominant genodermatosis of abnormal keratinization characterized by hyperkeratotic papules and plaques with a predilection for seborrheic areas. We report a case of a rare vesiculobullous variant of treatment-resistant Darier disease in a 55-year-old woman that failed topical tacrolimus and topical and oral glucocorticoids. Cetirizine was initiated at 10 mg daily and increased to 40 mg daily over four weeks, with resultant marked improvement of the patient’s burning sensation. A punch biopsy revealed a perivascular infiltrate of eosinophils. This patient’s symptomatic improvement with cetirizine, which has antagonizing properties against eosinophils, highlights the potential role of eosinophils in the pathogenesis of vesiculobullous Darier disease. We suggest that major basic protein secreted by eosinophils may propagate blister formation in vesiculobullous Darier disease by disrupting desmosomes.
Shivakumar, S. Mueller, P. Yamauchi, J. Weinberg, L. Kircik, J. Szepietowski, M. Goldust MD
ABSTRACT
Psoriasis is polygenic, interleukin (IL)-17 and IL-23 driven chronic relapsing inflammatory multisystem disease caused by a complex interplay of endogenous and environmental factors. The most common and distressing symptom in psoriasis is itch, adding significantly to the burden of disease. Although histamine has historically not been considered a key itch mediator in psoriasis, there is some evidence from the literature that antihistamines may be effective to reduce itch in psoriasis. This review focuses on the role of antihistamines in the management of itch in psoriasis. The literature search included peer-reviewed articles published in English language (clinical trials or scientific reviews). Studies were identified by searching electronic databases (MEDLINE and PubMed) until January 2021 and by reference lists of respective articles.
References
-
- U.S. FDA. Zyrtec® https://www.accessdata.fda.gov/drugsatfda_docs/label/2002/19835s15,%2020346s8lbl.pdf
- U.S. FDA. Claritin® https://www.accessdata.fda.gov/drugsatfda_docs/label/2000/20641s7lbl.pdf
- Naqvi A, Patel P, Gerriets V. Cetirizine. [Updated 2024 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549776/?utm_source.com
- Patel P, Akhondi H. Loratadine. [Updated 2025 Dec 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542278/
- Cookson H, Grattan C. An update on mast cell disorders. Clin Med (Lond). 2016;16(6):580-583. doi:10.7861/clinmedicine.16-6-580
- Pestelli, E et al. “Cetirizine reduces the number of tryptase-positive mast cells in psoriatic patients: a double-blind controlled study.” International journal of tissue reactions vol. 23,3 (2001): 97-103.
- D’Ovidio, R., Rossi, A. and Di Prima, T.M. (2010), THERAPEUTIC HOTLINE: Effectiveness of the association of cetirizine and topical steroids in lichen planus pilaris – an open-label clinical trial. Dermatologic Therapy, 23: 547-552. https://doi.org/10.1111/j.1529-8019.2010.01359.x
- Hsieh CY, Tsai TF. Use of H-1 Antihistamine in Dermatology: More than Itch and Urticaria Control: A Systematic Review. Dermatol Ther (Heidelb). 2021;11(3):719-732. doi:10.1007/s13555-021-00524-w
- Räßler, F., Lukács, J. and Elsner, P. (2016), Treatment of eosinophilic cellulitis (Wells syndrome) – a systematic review. J Eur Acad Dermatol Venereol, 30: 1465-1479. https://doi.org/10.1111/jdv.13706
- Wang, Jason F. et al. “Vesiculobullous Darier Disease Symptomatically Responsive to Cetirizine.” Journal of drugs in dermatology : JDD vol. 18,2 (2019): 213-214.
- Imaizumi A, Kawakami T, Murakami F, Soma Y, Mizoguchi M. Effective treatment of pruritus in atopic dermatitis using H1 antihistamines (second-generation antihistamines): changes in blood histamine and tryptase levels. J Dermatol Sci. 2003;33(1):23-29. doi:10.1016/S0923-1811(03)00132-4
- Rossi, A., Campo, D., Fortuna, M. C., Garelli, V., Pranteda, G., De Vita, G., … Carlesimo, M. (2018). A preliminary study on topical cetirizine in the therapeutic management of androgenetic alopecia. Journal of Dermatological Treatment, 29(2), 149–151. https://doi.org/10.1080/09546634.2017.1341610
- Zuberbier, Torsten et al. “The international EAACI/GA²LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria.” Allergy vol. 77,3 (2022): 734-766. doi:10.1111/all.15090
Did you enjoy this Therapeutic Cheat Sheet? You can find more here.