
Pediatric alopecia in children with kinky or curly hair presents unique diagnostic and management challenges. In a case-based session, Dr. Kenner-Bell reviewed common causes of hair loss in this population and highlighted the importance of early recognition, culturally sensitive counseling, and avoiding premature closure on traction alopecia as a diagnosis.
Case 1: Trichotillomania
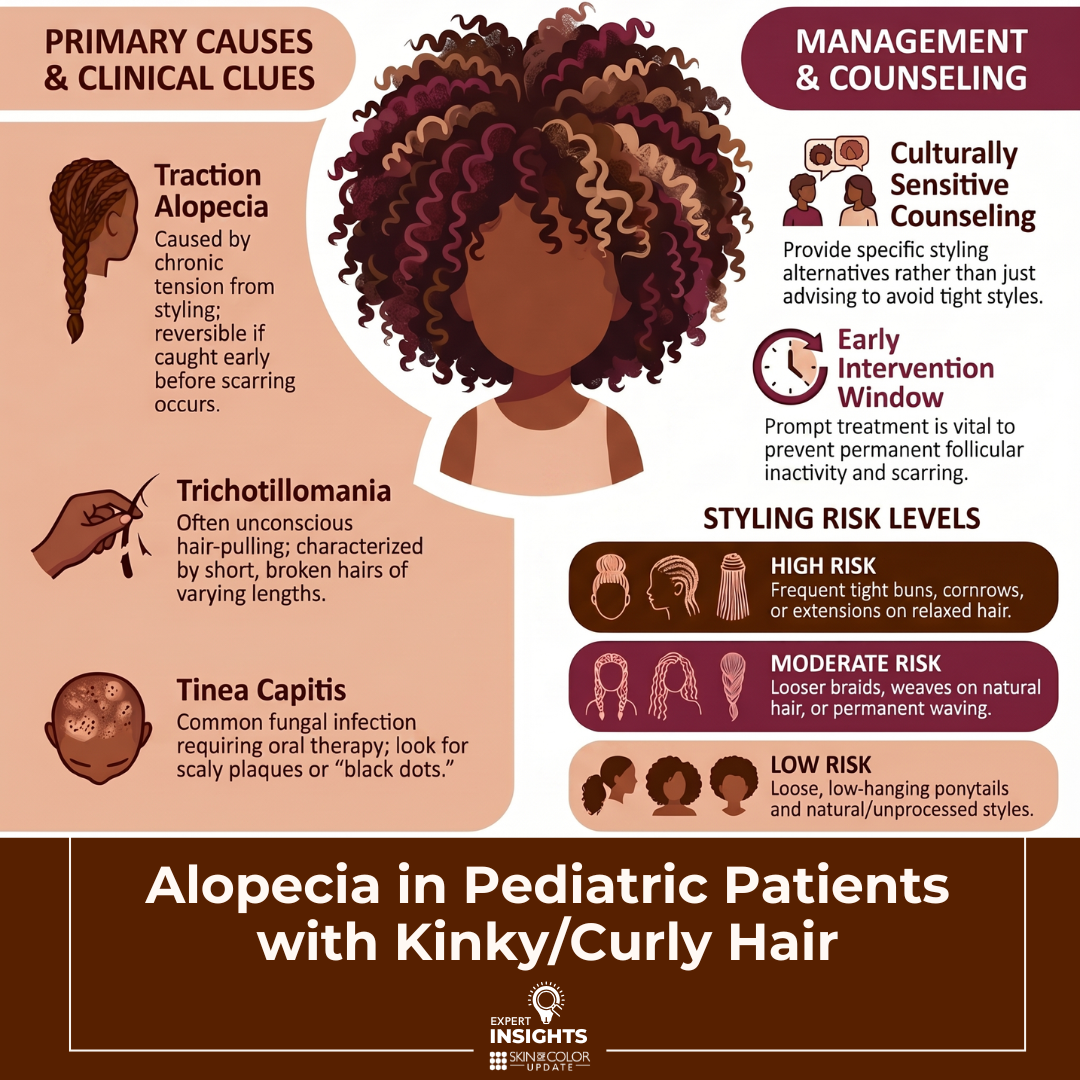
Trichotillomania may present in children from preschool age through adolescence and can involve plucking, pulling, twisting, or rubbing of the hair. The scalp is the most common site, but eyelashes and eyebrows may also be affected. This behavior often occurs unconsciously during quiet activities such as falling asleep, watching television, reading, or doing homework.
In younger children, hair-pulling may be associated with thumb-sucking, whereas in older children it may coexist with other compulsive behaviors such as nail biting or skin picking. Trichotillomania can also be associated with trichophagia, and a serious complication of this is trichobezoar.
Clinical clues to the diagnosis include short, broken hairs of varying lengths, a normal appearing scalp, irregularly shaped involvement on the anterior scalp, and incomplete hair loss without complete baldness. Lack of pain and a sense of relief or pleasure with pulling may be reported.
Most cases are self-limited and episodic. N-acetylcysteine has been used with some clinical evidence it can be helpful in certain patients. Between 50% and 75% of patients report mild psychiatric symptoms, therefore emotional support and behavioral modification strategies are important. Approximately 5% of patients, particularly tweens and teens, may have more significant psychiatric involvement. In these cases, cognitive behavioral therapy is useful, and referral for psychiatric evaluation may be warranted to consider tricyclic antidepressants (such as clomipramine) or SSRIs.
Case 2: Traction Alopecia
Traction alopecia can occur in all curl patterns but is more common in Black/African American patients due to hair styling practices that exert chronic tension on the hair. Early signs and symptoms include follicular-based papules and pustules, tension-related “tenting,” itching, tenderness, or a burning/stinging sensation, along with loss of terminal hairs with remaining vellus hairs.
Understanding hair care practices and the cultural factors behind them is essential. Counseling should be respectful and specific; simply saying “avoid tight hairstyles” is not sufficient. Early traction alopecia is reversible if tension is reduced and heat and chemical exposure are minimized. Low- to mid-potency topical steroids may help decrease inflammation. Patients should be educated that symptoms such as pain, stinging, crusting, or pimples indicate harmful traction.
Late-stage traction alopecia becomes scarring hair loss and is irreversible. The differential diagnosis includes congenital triangular alopecia (if present in early childhood), alopecia areata, and less commonly frontal fibrosing alopecia or central centrifugal cicatricial alopecia.
Recommended styling practices include alternating hairstyles, loosening braids especially along the hairline, avoiding prolonged braided styles, reducing heat and chemical relaxers, selecting larger braids or dreadlocks, removing extensions promptly if they cause discomfort, and incorporating breaks from styling.
Review of styling recommendations from the article “All hairstyles are not created equal: What the dermatologist needs to know about black hairstyling practices and the risk of traction alopecia (TA).”
High-risk hairstyles:
-
- Frequent tight buns or ponytails
- Tight braids/cornrows/dreadlocks
- Extensions or weaves (especially on relaxed hair)
- Any style causing pain, stinging, crusting, tenting, or pimples
Moderate-risk
-
- Looser braids/cornrows/dreadlocks
- Weaves or extensions applied to natural hair
- Wigs with cotton/nylon caps
- Permanent waving
Low-risk (preferred)
-
- Loose, low-hanging ponytails or buns
- Wigs with satin/silk caps
- Natural/unprocessed styles
Additional Practical Hair-Care Guidance
-
- Remove extensions or weaves every 3-4 weeks
- Avoid bonding glues, choose loosely sewn-in styles
- Give hair regular breaks from styling tension
- Limit heat and chemical relaxers
- Rotate braided styles and avoid keeping them longer than ~3 months
- Larger-diameter braids and locks reduce traction
Case 3: Tinea Capitis
Tinea capitis is one of the most common dermatophyte infections in children, especially among Black and Hispanic children. It typically affects ages 3-7 years but can occur even in infants, with boys being more commonly affected.
Clinical presentations include scaly plaques, diffuse scale, black dots, or inflammatory lesions. Trichoscopy showing corkscrew or comma hairs is supportive of diagnosis. Trichophyton tonsurans accounts for approximately 90% of cases in the U.S. and is human-to-human transmitted, whereas Microsporum canis commonly originates from cats.
Asymptomatic carriers are frequent reservoirs, so screening household contacts is encouraged.
Oral therapy is required for the treatment of tinea capitis:
-
- Griseofulvin: 20–25 mg/kg/day (microsize) for 6–12 weeks or 10–15 mg/kg/day (ultramicrosize); more effective for M. canis; must be taken with fatty food.
• Terbinafine: 3–6 mg/kg/day for 2–4 weeks; more effective for T. tonsurans; only in tablet form but may be crushed.
• Fluconazole: 5–12 mg/kg/day for 6 weeks; safe, including in children under 2 for certain indications.
• Itraconazole: 3–5 mg/kg/day for 4–6 weeks; not first line; useful in refractory M. canis.
- Griseofulvin: 20–25 mg/kg/day (microsize) for 6–12 weeks or 10–15 mg/kg/day (ultramicrosize); more effective for M. canis; must be taken with fatty food.
Adjunctive antifungal shampoos may reduce spread but can be drying to the hair shaft, so should be limited to every 1-2 weeks followed by conditioner. Use OTC selenium sulfide or zinc pyrithione formulations designed for kinky or curly hair.
Kerion formation carries an increased risk of scarring hair loss. Historically corticosteroids were used, but more recent evidence supports focusing primary therapy on antifungal treatment.
Case 4: Alopecia Areata
Twenty-four to sixty-five percent of alopecia areata cases occur before age 16. Patients who present with a few patches typically have excellent prognosis, whereas alopecia totalis/universalis has <10% full recovery. Recurrence occurs in approximately 30%.
Traditional therapies include topical/intralesional corticosteroids, topical minoxidil, topical immunotherapy, and phototherapy. Squaric acid dibutyl ester can take up to six months to show benefit, with Diphencyprone offering similar utility.
Emerging evidence supports the existence of a “window of opportunity” for more advanced therapy. Long-standing disease (>4 years for current episode) and higher baseline SALT scores predict poorer response to JAK inhibitors, supporting early initiation when appropriate.
New systemic options include:
-
- Ritlecitinib: Approved for patients ≥12 years; SALT ≤20 achieved in 17–28% of adolescents at 24 weeks; safety labs required at baseline and 4 weeks.
• Baricitinib: Effective and safe in limited pediatric data; SALT improvement of 68% at 24 weeks in patients ≤12 years.
- Ritlecitinib: Approved for patients ≥12 years; SALT ≤20 achieved in 17–28% of adolescents at 24 weeks; safety labs required at baseline and 4 weeks.
Low-dose oral minoxidil shows good safety but may cause hypertrichosis, hypotension, or headaches.
Case 5: Pediatric and Adolescent CCCA
Central centrifugal cicatricial alopecia can affect pediatric patients. Early hair breakage is a key sign. Direct questioning about symptoms is important. As in adults, delayed diagnosis leads to irreversible loss of follicles.
Take-Home Points
-
- Early recognition is key in pediatric alopecia as missing the treatment window can lead to permanent follicular inactivity.
• Hair-pulling disorders are common and often benign, but a subset require mental health support.
• Culturally informed, respectful counseling improves adherence and outcomes.
• Maintain a broad differential as traction alopecia is not the only cause of hair loss in kinky or curly hair.
• Tinea capitis must be treated orally; treatment should not be delayed pending culture.
- Early recognition is key in pediatric alopecia as missing the treatment window can lead to permanent follicular inactivity.
Sources:
Asfour, L., Bokhari, L., Bhoyrul, B., Eisman, S., Moussa, A., Rees, H., & Sinclair, R. D. (2023). Treatment of moderate-to-severe alopecia areata in pre-adolescent children with baricitinib. The British journal of dermatology, 189(2), 248–250. https://doi.org/10.1093/bjd/ljad118
Bookstaver, P. B., Watson, H. J., Winters, S. D., Carlson, A. L., & Schulz, R. M. (2011). Prophylactic ketoconazole shampoo for tinea capitis in a high-risk pediatric population. The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG, 16(3), 199–203. https://doi.org/10.5863/1551-6776-16.3.199
Castelo-Soccio L. (2014). Diagnosis and management of alopecia in children. Pediatric clinics of North America, 61(2), 427–442. https://doi.org/10.1016/j.pcl.2013.12.002
Cranwell, W., Meah, N., Wall, D., Bhoyrul, B., Laita, B., & Sinclair, R. D. (2024). Real-world effectiveness and safety of tofacitinib for alopecia areata: A retrospective cohort study of 202 patients. The Australasian journal of dermatology, 65(6), 505–513. https://doi.org/10.1111/ajd.14325
de Nicolas-Ruanes, B., Moreno-Arrones, O. M., Saceda-Corralo, D., Hermosa-Gelbard, A., Rodrigues-Barata, R., Gil-Redondo, R., Garcia-Mouronte, E., & Vañó-Galván, S. (2022). Low-dose oral minoxidil for treatment of androgenetic alopecia and telogen effluvium in a pediatric population: A descriptive study. Journal of the American Academy of Dermatology, 87(3), 700–702. https://doi.org/10.1016/j.jaad.2022.04.030
Elewski B. E. (2000). Tinea capitis: a current perspective. Journal of the American Academy of Dermatology, 42(1 Pt 1), 1–24. https://doi.org/10.1016/s0190-9622(00)90001-x
Grayson, C., & Heath, C. R. (2021). Counseling About Traction Alopecia: A “Compliment, Discuss, and Suggest” Method. Cutis, 108(1), 20–22. https://doi.org/10.12788/cutis.0297
Grigoryan, K. V., Tollefson, M. M., Olson, M. A., & Newman, C. C. (2019). Pediatric tinea capitis caused by Trichophyton violaceum and Trichophyton soudanense in Rochester, Minnesota, United States. International journal of dermatology, 58(8), 912–915. https://doi.org/10.1111/ijd.14352
Grover, C., Arora, P., & Manchanda, V. (2012). Comparative evaluation of griseofulvin, terbinafine and fluconazole in the treatment of tinea capitis. International journal of dermatology, 51(4), 455–458. https://doi.org/10.1111/j.1365-4632.2011.05341.x
Haskin, A., & Aguh, C. (2016). All hairstyles are not created equal: What the dermatologist needs to know about black hairstyling practices and the risk of traction alopecia (TA). Journal of the American Academy of Dermatology, 75(3), 606–611. https://doi.org/10.1016/j.jaad.2016.02.1162
Hughes, R., Chiaverini, C., Bahadoran, P., & Lacour, J. P. (2011). Corkscrew hair: a new dermoscopic sign for diagnosis of tinea capitis in black children. Archives of dermatology, 147(3), 355–356. https://doi.org/10.1001/archdermatol.2011.31
John, J. M., & Sinclair, R. (2023). Safety and tolerability of low-dose oral minoxidil in adolescents: A retrospective review. Journal of the American Academy of Dermatology, 88(2), 502–504. https://doi.org/10.1016/j.jaad.2022.06.1195
Jones, N. L., & Heath, C. R. (2021). Hair at the intersection of dermatology and anthropology: A conversation on race and relationships. Pediatric dermatology, 38 Suppl 2, 158–160. https://doi.org/10.1111/pde.14721
Koumantaki, E., Kakourou, T., Rallis, E., Riga, P., & Georgalla, S. (2001). Doubled dose of oral terbinafine is required for Microsporum canis tinea capitis. Pediatric dermatology, 18(4), 339–342. https://doi.org/10.1046/j.1525-1470.2001.01953.x
Koumantaki, E., Georgala, S., Rallis, E., & Papadavid, E. (2001). Microsporum canis tinea capitis in an 8-month-old infant successfully treated with 2 weekly pulses of oral itraconazole. Pediatric dermatology, 18(1), 60–62. https://doi.org/10.1046/j.1525-1470.2001.018001060.x
Tey, H. L., Tan, A. S., & Chan, Y. C. (2011). Meta-analysis of randomized, controlled trials comparing griseofulvin and terbinafine in the treatment of tinea capitis. Journal of the American Academy of Dermatology, 64(4), 663–670. https://doi.org/10.1016/j.jaad.2010.02.048
Williams, K.N., Olukoga, C., & Tosti, A. (2024). Evaluation of the Safety and Effectiveness of Oral Minoxidil in Children: A Systematic Review. Dermatology and Therapy, 14, 1709 – 1727.
Zampella, J. G., Kwatra, S. G., Blanck, J., & Cohen, B. (2017). Tinea in Tots: Cases and Literature Review of Oral Antifungal Treatment of Tinea Capitis in Children under 2 Years of Age. The Journal of pediatrics, 183, 12–18.e3. https://doi.org/10.1016/j.jpeds.2016.12.042
This summary was prepared by Dr. Courtney Hanna, who attended the session. The content reflects the resident’s notes and interpretations, may contain errors, and is provided for educational purposes only.
Did you enjoy this article? Find more on Skin of Color Dermatology here.