
Authors Jacob Reinhart MD, Matthew Willett MD, and Neil Gibbs MD present a case of psoriatic lesions precipitated by an upper arm tattoo.
Psoriasis is a common dermatologic skin condition with a variety of morphologic presentations. These variations include the less common hyperkeratotic form, psoriasis ostracea, defined as having pronounced adherent scales (skin lesions) resembling an oyster shell. Of the ostraceous cases that have been reported in the literature, many occur as generalized outbreaks in patients with long-standing history of psoriasis. Rarely does this remarkable variant occur as a direct flare from a cutaneous insult. In these situations, when a pre-existing dermatosis appears in response to a traumatic insult to skin, the process is referred to as the Koebner phenomenon. In addition to lichen planus and vitiligo, psoriasis is a commonly known condition that can present as a Koebner reaction. In this atypical case, the authors present a 21-year-old male with remarkable ostraceous psoriatic lesions precipitated by an upper arm tattoo, demonstrating the Koebner phenomenon.
Introduction
A 21-year-old Naval active duty male presented for his first dermatologic evaluation with the chief complaint of a six-week history of mildly pruritic cutaneous lesions involving his face and recently tattooed right upper arm. His initial skin manifestation was a new-onset greasy, scaling rash over his forehead, eyebrows, and bilateral cheeks. Two weeks subsequent to developing his facial lesions, after acquiring a large upper arm tattoo, he observed a reaction of similarly appearing red, scaling plaques throughout the recently tattooed region.
The condition continued to increase in severity in both his tattooed arm, as well as face, over the next six weeks. The patient was initially treated by his primary care provider with oral antibiotics for a presumed bacterial infection, but was subsequently referred to Naval Medical Center San Diego Dermatology for failure to improve.
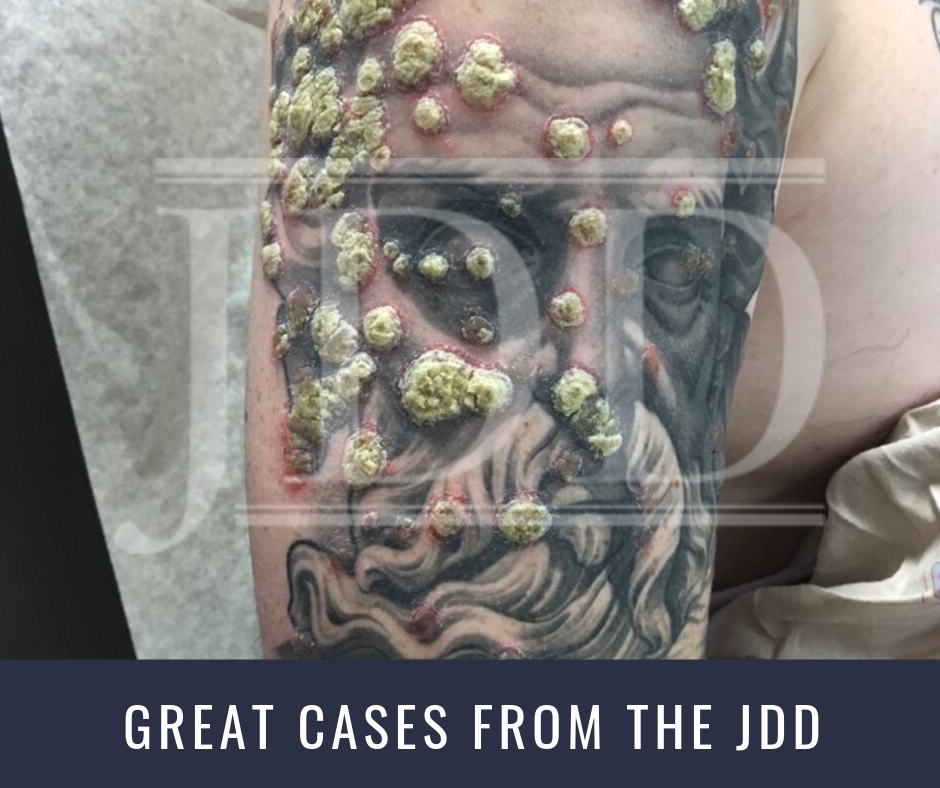
Dermatologic exam showed significant erythematous nodules with pronounced ostraceous scale overlying a right upper arm tattoo (Figures 1 and 2). Notably, the configuration of scaled lesions directly outlined ink markings within the tattoo. In addition, he displayed multiple erythematous plaques with adherent ‘greasy’ yellow scale on forehead, bilateral eyebrows, glabella, bilateral cheeks, upper cutaneous lip, and upper back (Figure 3).


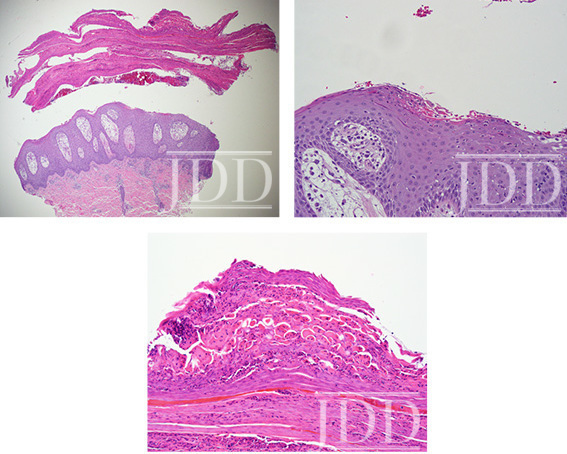
The differential diagnoses for scattered erythematous plaques with adherent scale included psoriasis, seborrheic dermatitis, tinea corporis, and atypical mycobacterial infection. A punch biopsy from the patient’s right upper arm revealed a hyperkeratotic stratum corneum layer, Munro’s microabscesses, and elongation of the rete ridges, consistent with a diagnosis of psoriasis (Figures 4-6). The patient was subsequently treated with desonide 0.05% topical cream twice daily for 7 days and then transitioned to pimecrolimus 1% cream twice daily with marked subjective improvement in symptoms.
Discussion
Ostraceous psoriasis is one of several hyperkeratotic variants of psoriasis to include rupioid and elephantine which assume distinctive scaling appearances. The ostraceous form is named for its circular or oval-shaped lesions consisting of thick, adherent scales resembling an oyster shell, often with a characteristic concave center. Although it can be distinguished from the rupioid form, which has dark, concentric layers that resemble syphilitic rupia, the two terms were previously classified together under psoriasis exudativa.1 Thick layers formed by serous fluid are believed to be responsible for the formation of these exudative crusts.
Both hyperkeratotic forms of psoriasis are marked for their excessively thick, scaling plaques that have often been considered resistant to topical forms of therapy.2,3Management of Koebner reactions focuses treatment on the underlying condition; however, this creates challenges as topical medications are often the basis of treatment for psoriasis. It should be noted that patient compliance has been suggested as a confounding variable in the response to treatment.4 Some cases have reported improvement and even resolution of these hyperkeratotic psoriatic lesions solely with topical treatment.5
This case presents a unique occurrence of ostraceous psoriasis appearing in response to a recent tattoo. The Koebner phenomenon describes a dermatologic response of a pre-existing dermatosis such as psoriasis in a new distribution following a traumatic insult. The phenomenon has been reported in up to 25% of psoriasis cases, with typical onset of symptoms within 10-20 days of inciting event.6Cutaneous insults that have been shown to spark a Koebner reaction range from sunburns to minor scrapes, and as seen in this case, the tattooing process. While psoriasis has previously been shown to Koebnerize following recent tattoos, the more common presentation of plaque psoriasis seems to be a standard reaction.7 The pronounced ostraceous lesions identified in this case are a striking Koebner response triggered by the tattoo process.
With increasing popularity of tattoos, one study estimating 24%, a comprehensive risk assessment needs to be taken.8 This tattoo incidence is even higher within military population, with estimates of 36%.9 Beyond implicit risks of infection and allergic or irritant reactions, Koebnerization of underlying dermatologic conditions should be fully realized by individuals before pursing tattoos. Patients with any degree of psoriasis should be cautioned by their providers about the risk of triggering new lesions with the tattooing process. For providers, early recognition of tattoo complications is essential and Koebnerization should be included in the differential diagnosis of dermatologic reactions precipitated by a tattoo.
References
- Salamon M, Omulecki A, Sysa-Jedrzeejowska A, et al. Psoriasis rupioides: a rare variant of a common disease. Cutis. 2011;88(3):135-7.
- Mesquita LSU, Sherlock J, Portugal FM, et al. Case for diagnosis. Ostraceous psoriasis: a case report. An Bras Dermatol. 2014;89(5):841-2.
- Arias-Santiago SA, Naranjo-Sintes R. Images in clinical medicine. Generalized ostraceous psoriasis. N. Engl. J. Med. 2010; 362(2):155.
- Feldman SR, Brown KL, Heald P. ‘Coral reef’ psoriasis: a marker of resistance to topical treatment. J Dermatolog Treat. 2008;19(5):257-8.
- Wu JJ, Caperton C. Images in clinical medicine. Psoriasis flare from Koebner’s phenomenon after acupuncture. N. Engl. J. Med. 2013; 368 (17): 1635.
- Weiss G, Shemer A, Trau H. The Koebner phenomenon: review of the literature. J Eur Acad Dermatol Venereol. 2002;16:241-8.
- Arias-Santiago, S, Espineira-Carmona MJ, Aneiros-Fernandez J. The Koebner phenomenon: psoriasis in tattoos. Can Med Ass J. 2013;185(7):585.
- Laumann AE, Derick AJ. Tattoos and body piercings in the United States: A national data set. J Am Acad Dermatol. 2006;55:413-21.
- Armstrong ML, Roberts AE, Koch JR, et al. Motivation for contemporary tattoo removal: a shift in identity. Arch Dermatol. 2008;144(7):879–84.
Source: Reinhart, J., MD, Willet, M., MD, & Gibbs,N., MD. (2019). Ostraceous Psoriasis Presenting as Koebner Phenomenon in a Tattoo. Journal of Drugs in Dermatology, 18(8), 825-826. Retrieved August 14, 2019, from https://jddonline.com/articles/dermatology/S1545961619P0697X/1/.
Content and images used with permission from the Journal of Drugs in Dermatology.
Adapted from original article for length and style.
Did you enjoy this case report? Find more here.