
Abstract
Botulinum toxin type A (BTA) is a neurotoxic protein that prevents the release of neurotransmitters from presynaptic nerves and has shown promise in treating neuropathic pain. Recently, BTA has been used to treat painful keloids and scars. We present a patient with refractory neuropathic pain in a normotrophic spread-scar treated with the injection of BTA.
A 47-year-old Caucasian female with a history of invasive melanoma of the left upper arm presented with pain in her excision scar, which she described as a “pins and needles” sensation alternating with a dull, deep ache. She had previously tried topical lidocaine, topical and intralesional steroids, and oral gabapentin without improvement. We treated the patient with 50 U of onabotulinumtoxinA intradermally at 1-1.5 cm intervals within and immediately around the perimeter of the scar. At 1-week follow-up, she reported a 10% decrease in her pain. Four weeks after the procedure, she reported a 50% decrease in pain with smoothening of the scar surface, which has been durable for over 5 months. Scar pain can significantly impair quality of life and treatment protocols have not been established for normotrophic scars. Many trials have focused on improving appearance and reducing symptoms in hypertrophic and keloid scars, but few have evaluated therapies for normotrophic scars. BTA has been studied as a treatment for painful hypertrophic and keloid scars with promising results. Our patient had a marked reduction in pain and improvement in scar texture at 1-month follow-up, which has been maintained thus far, indicating that intradermal BTA may be a simple and useful tool in treating painful normotrophic scars.
Introduction
Botulinum toxin type A (BTA) is a neurotoxic protein that binds to soluble N-ethylmaleimide-sensitive factor attachment protein receptor, preventing release of neurotransmitters from presynaptic nerves.1 BTA is hypothesized to directly exert analgesic properties by reducing release of mediators like substance P, glutamate, and calcitonin gene related peptide (CGRP); in one mouse model of neuropathic pain, a single injection of BTA was shown to significantly reduce allodynia for up to 3 weeks.1,2Clinically, BTA has shown promise in treating disorders characterized by neuropathic pain, including trigeminal neuralgia, postherpetic neuralgia, diabetic neuropathy, as well as postsurgical neuropathic pain from thoracotomies, carpal tunnel surgery and more.1,3-5 Recently, there have also been successful reports using BTA to treat painful keloid scars and postoperative Mohs scars.6-8 Here, we present a patient with refractory neuropathic pain in a normotrophic spread-scar successfully treated with injection of BTA.
Case
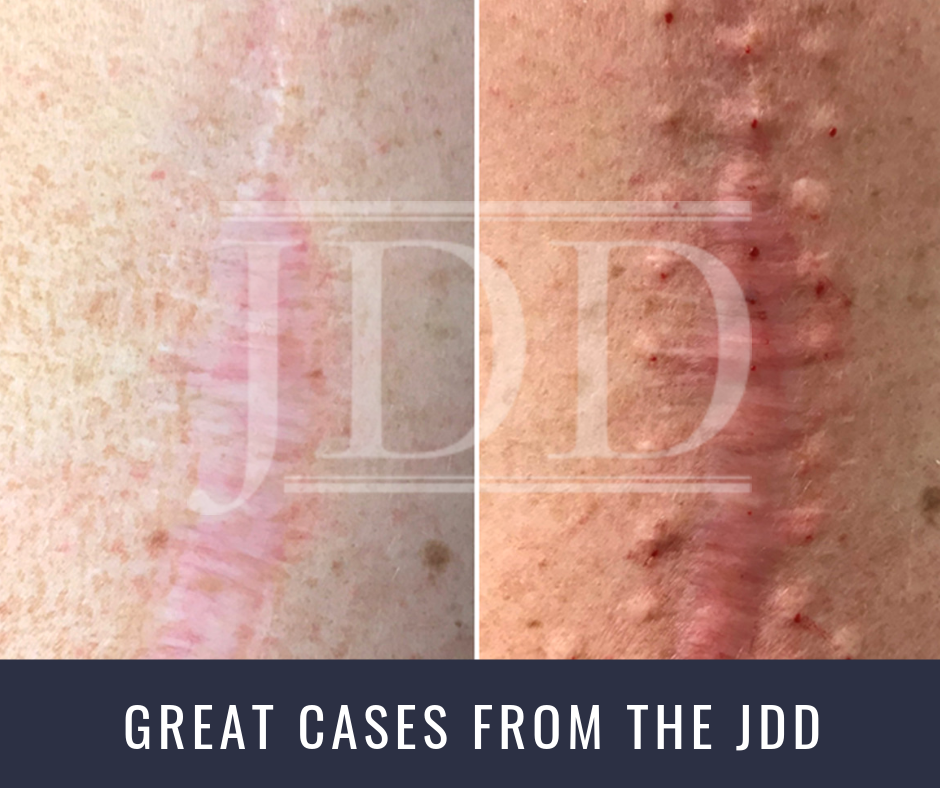
A 47-year-old Caucasian female with a history of melanoma of the left upper arm presented presented with pain at the site of her excision scar. Her melanoma was removed by wide local excision 5 years prior; after the incision healed she began to experience constant pain in the scar. She described the pain as a “pins and needles” sensation that alternated with a dull, deep ache. The pain significantly impacted her quality of life, waking her from sleep and preventing her from lying on her left side. She also noticed surface changes of the skin that left the scar uneven to the touch. She had previously tried topical lidocaine and topical and intralesional steroids without any effect. She had used gabapentin 100 mg three times daily but stopped taking it due to sedation. On physical examination there was a 15-cm normotrophic, slightly pink surgical scar with prominent spreading of the inferior two-thirds of the scar on the left upper lateral arm (Figure 1A).
To treat the scar, 50 units of BTA were injected intradermally at 1-1.5 cm intervals within and immediately around the perimeter of the scar (Figure 1B). The patient tolerated the procedure well with minimal pain and no complications. At a 1-week follow-up, there was a self-reported 10% decrease in pain associated with the scar. Four weeks after the procedure, the patient reported a 50% decrease in her pain from baseline along with relaxation and smoothening of the scar surface. These effects have been sustained greater than 5 months after treatment.

Discussion
Mature scars, especially hypertrophic and keloid scars, can negatively impact patients’ quality of life through cosmetic disfigurement, pain, itching, and restriction of mobility.9,10Neuropathic pain in hypertrophic and keloid scars is partially mediated by neuropeptides like CGRP and substance P; recent data have implicated these neurotransmitters as a source of pain in normotrophic scars as well.1,11 Our case also illustrates that tension vectures from scar contracture may also play a role in persistent neuropathic scar pain.
Various therapies have been studied for the prevention and treatment of scars. Many trials have focused on improving cosmetic appearance and reducing symptoms in hypertrophic and keloid scars, but less emphasis has been placed on therapies for normotrophic scars. Current guidelines cite compression and occlusive therapy, intralesional steroids, cryotherapy, laser therapy and surgical excision as first-line therapies for treating keloid and hypertrophic scars.12,13 Emerging therapies continue to be studied, including 5-fluorouracil, imiquimod, tacrolimus, retinoic acid, and verapamil.13 BTA has been studied as a monotherapy for treatment of scars with promising results. Multiple, small randomized controlled trials have shown BTA to be as effective as intralesional steroid injections at reducing volume of hypertrophic scars, improving pliability, erythema and itching.14 Studies of postoperative scar prevention with BTA have also shown promise.15 Regarding neuropathic pain, only one study and several case reports have demonstrated pain reduction in scars after injection with BTA.4,6,7 A single case report also described a durable reduction in neuropathic scar pain after 1 treatment of BTA for a 6-month-old Mohs surgery scar.8 Our patient described a pins and needles sensation at her melanoma excision scar consistent with neuropathic pain, which was refractory to multiple other treatments. Given the successful use of BTA in conditions with neuropathic pain and the few reports of pain reduction in keloid and Mohs scars, we hypothesized that BTA injection may yield therapeutic benefit in our patient as well. Our patient had marked, durable reduction in scar pain symptoms after treatment, indicating that BTA may be a viable treatment for painful normotrophic scars. However, further studies are needed to help determine the efficacy of BTA in treating painful hypertrophic, keloid, and normotrophic scars.
References:
- Francisco GE, Tan H, Green M. Do botulinum toxins have a role in the management of neuropathic pain?: a focused review. Am J Phys Med Rehabil. 2012;91:899-909.
- Luvisetto S, Marinelli S, Cobianchi S, Pavone F. Anti-allodynic efficacy of botulinum neurotoxin A in a model of neuropathic pain. Neuroscience. 2007;145:1-4.
- Yuan RY, Sheu JJ, Yu JM, et al. Botulinum toxin for diabetic neuropathic pain: a randomized double-blind crossover trial. Neurology. 2009;72:1473-1478.
- Fabregat G, Asensio-Samper J, Palmisani S, et al. Subcutaneous botulinum toxin for chronic post-thoracotomy pain. Pain Pract. 2013;13:231-234.
- Ranoux D, Attal N, Morain F, Bouhassira D. Botulinum toxin type A induces direct analgesic effects in chronic neuropathic pain. Ann Neurol. 2008;64:274- 283.
- Uyesugi B, Lippincott B, Dave S. Treatment of a painful keloid with botulinum toxin type A. Am J Phys Med Rehabil. 2010;89:153-155.
- Shaarawy E, Hegazy RA, Abdel Hay RM. Intralesional botulinum toxin type A equally effective and better tolerated than intralesional steroid in the treatment of keloids: a randomized controlled trial. J Cosmet Dermatol. 2015;14:161-166.
- DePry JL, Mann M. Successful treatment of postoperative pain after Mohs micrographic surgery with onabotulinum toxin A. Dermatol Surg. 2017;43:1491-1494.
- Bock O, Schmid-Ott G, Malewski P, Mrowietz U. Quality of life of patients with keloid and hypertrophic scarring. Arch Dermatol Res. 2006;297:433- 438.
- Gurtner GC, Neligan PC. Vol 1: Principles. Plastic Surgery. 4th ed. London: Elsevier. 2017.
- Powers M, Ozog D, Chaffins M. Scar histopathology and morphologic classification. In: Krakowski AC, Shumaker PR, eds. The Scar Book: Formation, Mitigation, Rehabilitation, and Prevention. Philadelphia: Wolters Kluwer. 2017:59-71.
- Gold MH, McGuire M, Mustoe TA, et al. Updated international clinical recommendations on scar management: part 2 – algorithms for scar prevention and treatment. Dermatol Surg. 2014;40:825-831.
- Berman B, Maderal A, Raphael B. Keloids and hypertrophic scars: pathophysiology, classification, and treatment. Dermatol Surg. 2017;43:S3-S18.
- Kim YS, Hong ES, Kim HS. Botulinum toxin in the field of dermatology: novel indications. Toxins (Basel). 2017;9:E403.
- Giordano CN, Matarasso SL, Ozog DM. Injectable and topical neurotoxins in dermatology: indications, adverse events, and controversies. J Am Acad Dermatol. 2017;76:1027-1042.
Source:
Schuler, A., BS, Veenstra, J., MD PhD, & Ozog, D., MD. (2019). Battling Neuropathic Scar Pain With Botulinum Toxin. Journal of Drugs in Dermatology, 18(9), 937-938. Retrieved August 31, 2019, from https://jddonline.com/articles/dermatology/S1545961619P0937X/1/
Content and images used with permission from the Journal of Drugs in Dermatology
Did you enjoy this case report? Find more here.