
Everyday Health recently addressed the “invisible burden of atopic dermatitis” – the impact of the condition on a patient’s mental health. As a psychophysiological disorder, psychological stress can worsen atopic dermatitis (AD) flares, which in turn creates more inflammation in the body that stresses the nervous system. Chronic itch and sleep disturbances compound the distress, contributing to anxiety, depression, and irritability. Yet patients may hesitate to discuss their mental health with their dermatologists, and dermatologists may not know how to raise the topic with their patients.
To better understand AD and its mental health effects, I interviewed Mohammad Jafferany, MD, DFAPA, MCPS, professor of psychodermatology, psychiatry, and behavioral sciences at the Covenant HealthCare College of Medicine at Central Michigan University. Dr. Jafferany is president of the Association for Psychocutaneous Medicine of North America and president of World Psychodermatology Day.
You are trained in both dermatology and psychiatry. How do these fields intersect in your patient care, particularly when caring for patients with AD?
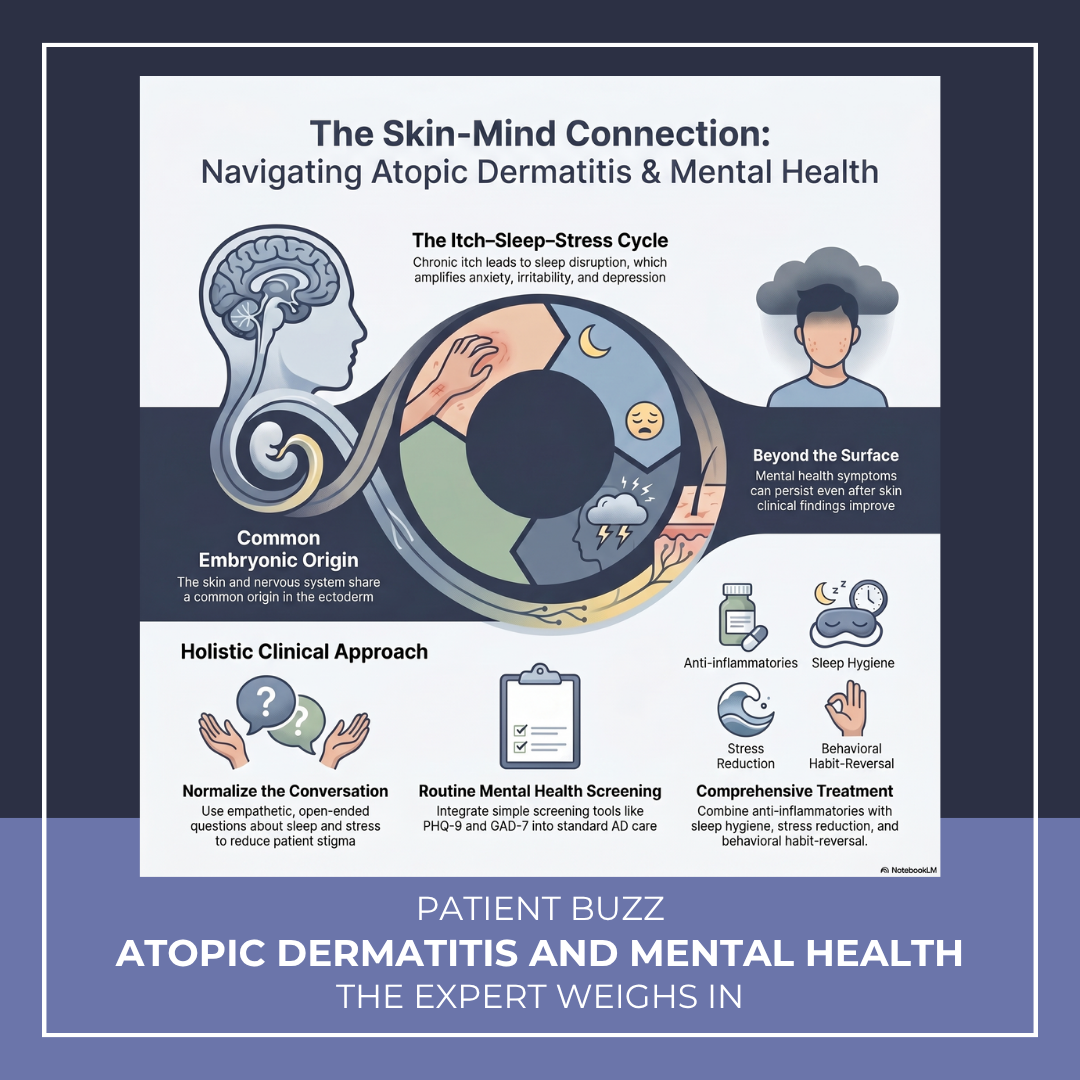
There is a direct bidirectional relationship between skin and nervous system from their common embryonic origin from ectoderm. Therefore, dermatology and psychiatry intersect closely in atopic dermatitis like many other psychodermatological disorders. Stress, anxiety, and poor sleep can worsen itch and flares, while chronic itch and visible disease can lead to significant psychological burden, including anxiety and depression. In my care, I routinely screen for sleep and mental health concerns, address both the biological and behavioral aspects of itch (including the itch–scratch cycle), and educate patients about the stress–skin connection. I also incorporate simple strategies like sleep hygiene and stress reduction and collaborate with mental health professionals when needed.
What’s unique about the mental health impact of AD compared with other inflammatory skin diseases?
The most common determinants in AD are itch, sleep disruption, and early onset. Compared with other inflammatory skin diseases, AD patients have relentless itch that drives a powerful itch–scratch cycle. This leads to chronic sleep deprivation, amplifying mood symptoms like anxiety, irritability, and depression. AD also often starts in childhood, so patients and families may deal with years of disrupted sleep and stress from early developmental stages. Besides that, the visibility and unpredictability of flares contribute to heightened psychosocial burden and stigma.
Patients may hesitate to disclose mental health challenges to a dermatologist. What’s your approach for broaching the topic?
I bring it up routinely and normalize it as part of AD care, so patients don’t feel singled out. I use simple, layman language and try to make them understand the connection between stress and flare ups. Then I ask brief, open-ended questions about sleep, stress, and how the condition is affecting daily life. I use a very empathetic and non-judgmental approach. I ask questions like: “Sometimes stress or poor sleep can make flares worse, and we can treat both sides.” If patients acknowledge then I validate their experience and offer a simple explanation of itch-scratch cycle, framing it as part of a comprehensive plan of care rather than something separate.
What are some underrecognized signs of mental health challenges in patients with AD?
Common underrecognized signs include chronic sleep disturbance, disproportionate itch or distress relative to skin findings, and apparent nonadherence or non-compliance with treatment, possibly due to burnout or low mood. Patients may also have stress-triggered flares, social withdrawal, irritability (especially in children), or habitual scratching that goes beyond inflammation. Some minimize their symptoms despite significant quality-of-life impact. Recognizing these patterns can help guide more holistic care for these patients.
What tools and supports do you recommend for AD patients who have mental health challenges?
These patients require psychoeducation and explanation of their symptoms in a clear and common language, avoiding medical jargon. I commonly use simple screening tools such as PHQ-9 (Patient Health Questionnaire-9) and GAD-7 (Generalized Anxiety Disorder-7 item) to check the severity of depression and anxiety respectively. Besides that, I educate about the itch–stress–sleep cycle, and behavioral strategies such as sleep hygiene, stress reduction techniques, and habit-reversal for scratching. Moisturizing routines and consistent anti-inflammatory treatment help reduce itch, which in turn improves sleep and mood. I also encourage use of support resources (patient groups or digital apps for mindfulness and stress), and when needed, collaboration with mental health professionals for psychotherapy or medications, such as selective serotonin reuptake inhibitors (SSRIs), which help with anxiety and depression both.
How much should mental health factor in AD treatment decisions?
Addressing psychological factors is a fundamental part of a comprehensive treatment plan for AD patients. The impact of itch, sleep loss, and psychosocial burden often drives overall disease severity as much as the visible skin findings. For example, patients with moderate skin disease but severe sleep disruption or anxiety may warrant earlier escalation to systemic or targeted therapies. Similarly, addressing behavioral factors (like the itch–scratch cycle) and supporting mental health can significantly improve outcomes alongside medical treatment. In practice, I weigh quality of life, sleep, and emotional impact alongside clinical severity when choosing therapies.
What misconceptions do dermatology clinicians often have about mental health and AD?
A common misconception is that mental health issues in atopic dermatitis (AD) are secondary or only relevant in severe disease, when in reality they can be present at any stage and often drive overall burden. Clinicians may also underestimate how profoundly itch and sleep loss affect mood and quality of life. Another dilemma is labeling patients as nonadherent or non-compliant without recognizing underlying factors like depression, anxiety, or treatment fatigue and burn out. Some also overlook the behavioral component of the itch–scratch cycle or feel that mental health falls outside the scope of dermatology. Here comes the importance of psychodermatology awareness and training in dermatology clinicians.
What else should dermatology clinicians know about mental health and AD?
Dermatology clinicians should recognize that mental health in atopic dermatitis (AD) is bidirectional and often underreported. Patients may not volunteer concerns unless directly asked. The clinicians need to be suspicious and ask the patient directly in a non-judgmental way. The burden extends beyond the patient to families and caregivers, especially in pediatric cases. Mental health symptoms can persist even when skin improves, so ongoing psychiatric assessment is important. Small, consistent interventions, such as improving sleep, validating patient experiences, and addressing the itch–scratch cycle, can have a meaningful impact. Finally, integrating mental health into routine care doesn’t require extensive time; even brief screening of anxiety and depression by questionnaires, such as PHQ-9 and GAD-7, and appropriate referral can significantly improve overall outcomes.
Did you enjoy this Patient Buzz expert commentary? You can find more here.