
Alitretinoin (9-cis-retinoic acid) is a naturally occurring endogenous retinoid that in gel form is FDA approved for AIDs-related localized cutaneous Kaposi’s sarcoma (KS)1. As compared to other topical retinoids, alitretinoin is unique in that it binds to all known intracellular retinoid receptors (RARs and RXRs), allowing it to exert anti-proliferative and apoptotic effects, particularly useful in treating Kaposi’s sarcoma1. Alitretinoin gel is a safe, highly effective, and non-invasive treatment, joining other localized KS therapies such as radiation, surgical excision, cryosurgery or intralesional therapies1. We continue our series, Therapeutic Cheat Sheet, with a closer look at alitretinoin gel.
Alitretinoin Gel Therapeutic Cheat Sheet
Compiled by: Adam Rosenfeld MD | Reviewed by: Adam Friedman, MD
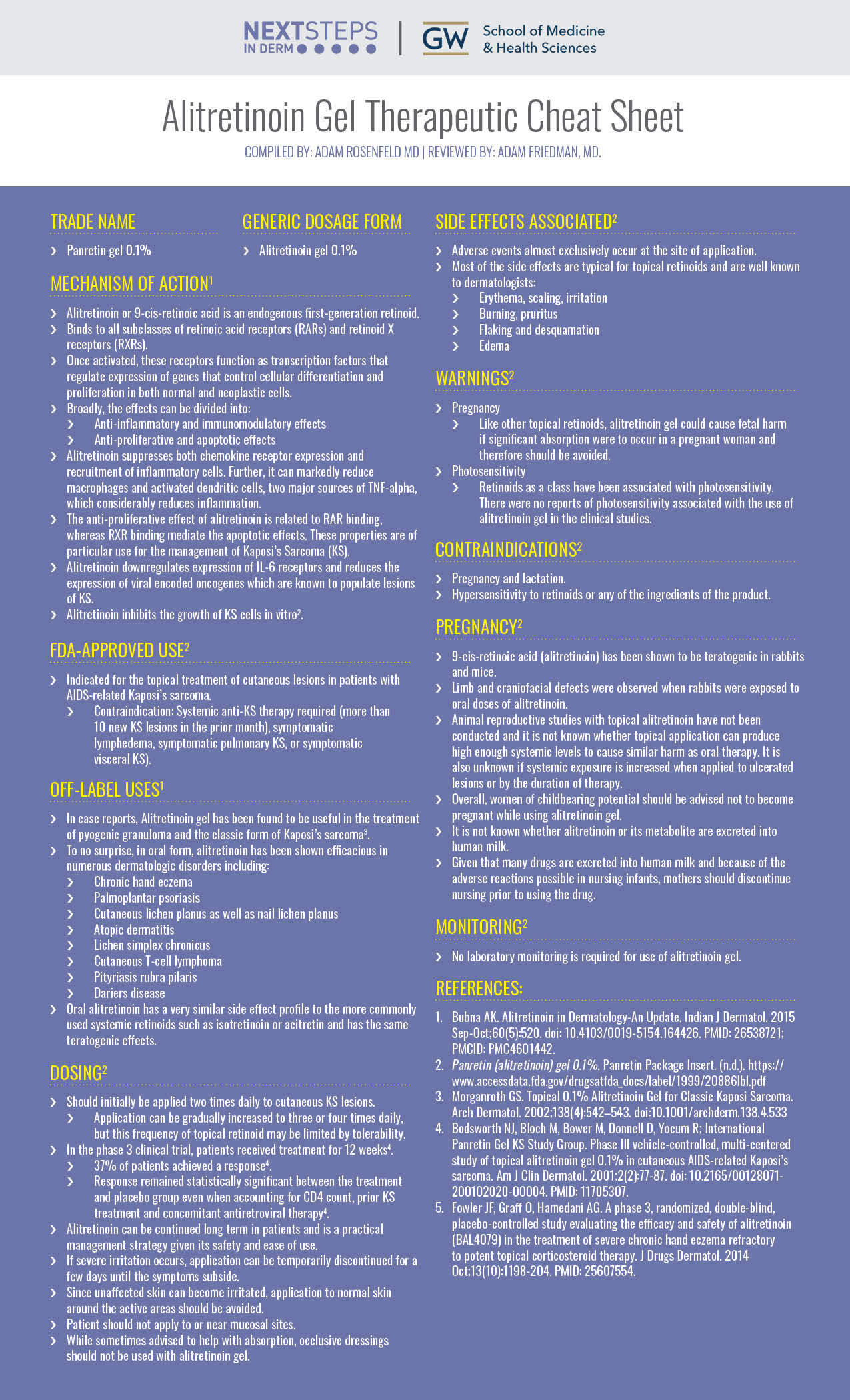
TRADE NAME
-
- Panretin gel 0.1%
GENERIC DOSAGE FORM
-
- Alitretinoin gel 0.1%
MECHANISM OF ACTION1
-
- Alitretinoin or 9-cis-retinoic acid is an endogenous first-generation retinoid.
- Binds to all subclasses of retinoic acid receptors (RARs) and retinoid X receptors (RXRs).
- Once activated, these receptors function as transcription factors that regulate expression of genes that control cellular differentiation and proliferation in both normal and neoplastic cells.
- Broadly, the effects can be divided into:
- Anti-inflammatory and immunomodulatory effects
- Anti-proliferative and apoptotic effects
- Alitretinoin suppresses both chemokine receptor expression and recruitment of inflammatory cells. Further, it can markedly reduce macrophages and activated dendritic cells, two major sources of TNF-alpha, which considerably reduces inflammation.
- The anti-proliferative effect of alitretinoin is related to RAR binding, whereas RXR binding mediate the apoptotic effects. These properties are of particular use for the management of Kaposi’s Sarcoma (KS).
- Alitretinoin downregulates expression of IL-6 receptors and reduces the expression of viral encoded oncogenes which are known to populate lesions of KS.
- Alitretinoin inhibits the growth of KS cells in vitro2.
FDA-APPROVED USE2
-
- Indicated for the topical treatment of cutaneous lesions in patients with AIDS-related Kaposi’s sarcoma.
- Contraindication: Systemic anti-KS therapy required (more than 10 new KS lesions in the prior month), symptomatic lymphedema, symptomatic pulmonary KS, or symptomatic visceral KS).
- Indicated for the topical treatment of cutaneous lesions in patients with AIDS-related Kaposi’s sarcoma.
OFF-LABEL USES1
-
- In case reports, Alitretinoin gel has been found to be useful in the treatment of pyogenic granuloma and the classic form of Kaposi’s sarcoma3.
- To no surprise, in oral form, alitretinoin has been shown efficacious in numerous dermatologic disorders including:
- Chronic hand eczema
- Palmoplantar psoriasis
- Cutaneous lichen planus as well as nail lichen planus
- Atopic dermatitis
- Lichen simplex chronicus
- Cutaneous T-cell lymphoma
- Pityriasis rubra pilaris
- Dariers disease
- Oral alitretinoin has a very similar side effect profile to the more commonly used systemic retinoids such as isotretinoin or acitretin and has the same teratogenic effects.
DOSING2
-
- Should initially be applied two times daily to cutaneous KS lesions.
- Application can be gradually increased to three or four times daily, but this frequency of topical retinoid may be limited by tolerability.
- In the phase 3 clinical trial, patients received treatment for 12 weeks4.
- 37% of patients achieved a response4.
- Response remained statistically significant between the treatment and placebo group even when accounting for CD4 count, prior KS treatment and concomitant antiretroviral therapy4.
- Alitretinoin can be continued long term in patients and is a practical management strategy given its safety and ease of use.
- If severe irritation occurs, application can be temporarily discontinued for a few days until the symptoms subside.
- Since unaffected skin can become irritated, application to normal skin around the active areas should be avoided.
- Patient should not apply to or near mucosal sites.
- While sometimes advised to help with absorption, occlusive dressings should not be used with alitretinoin gel.
- Should initially be applied two times daily to cutaneous KS lesions.
SIDE EFFECTS ASSOCIATED2
-
- Adverse events almost exclusively occur at the site of application.
- Most of the side effects are typical for topical retinoids and are well known to dermatologists:
- Erythema, scaling, irritation
- Burning, pruritus
- Flaking and desquamation
- Edema
WARNINGS2
-
- Pregnancy
- Like other topical retinoids, alitretinoin gel could cause fetal harm if significant absorption were to occur in a pregnant woman and therefore should be avoided.
- Pregnancy
-
- Photosensitivity
- Retinoids as a class have been associated with photosensitivity. There were no reports of photosensitivity associated with the use of alitretinoin gel in the clinical studies.
- Photosensitivity
CONTRAINDICATIONS2
-
- Pregnancy and lactation.
- Hypersensitivity to retinoids or any of the ingredients of the product.
PREGNANCY2
-
- 9-cis-retinoic acid (alitretinoin) has been shown to be teratogenic in rabbits and mice.
- Limb and craniofacial defects were observed when rabbits were exposed to oral doses of alitretinoin.
- Animal reproductive studies with topical alitretinoin have not been conducted and it is not known whether topical application can produce high enough systemic levels to cause similar harm as oral therapy. It is also unknown if systemic exposure is increased when applied to ulcerated lesions or by the duration of therapy.
- Overall, women of childbearing potential should be advised not to become pregnant while using alitretinoin gel.
- It is not known whether alitretinoin or its metabolite are excreted into human milk.
- Given that many drugs are excreted into human milk and because of the adverse reactions possible in nursing infants, mothers should discontinue nursing prior to using the drug.
MONITORING2
-
- No laboratory monitoring is required for use of alitretinoin gel.
Alitretinoin gel is a pan retinoid receptor agonist that is FDA approved for AIDs-related localized cutaneous KS. It can be used as first line therapy but is also extremely useful when other modalities, such as radiation or excision are not practical. While other systemic retinoids are widely used in dermatology, there have not been large studies evaluating oral alitretinoin. As expected, oral alitretinoin has been shown to be efficacious in the off-label setting for numerous dermatologist conditions, which includes its use in Europe for recalcitrant hand eczema1. While it may prove to be valuable in other retinoid responsive dermatosis, it is vital for dermatologists to be aware of its efficacy in KS.
Further Reading
Published in Journal of Drugs in Dermatology
Joseph F Fower, Ole Graff, Abbas G Hamedani
Abstract: Severe chronic hand eczema (sCHE) is a persistent, disfiguring disease that responds poorly to conventional treatment and causes substantial physical and psychological disability. The objective of this study was to evaluate efficacy and safety of oral alitretinoin in sCHE in a Phase 3, multicenter, randomized, double-blind, placebo-controlled, parallel-group study comparing alitretinoin with placebo. Efficacy was assessed every 4 weeks during treatment and 4 weeks after end of treatment (EOT, 24 weeks); responders were assessed every 4 weeks for a further 48 weeks after EOT. The study was conducted at academic and private dermatology centers. The participants were 596 patients with sCHE refractory to potent topical corticosteroids. Patients were treated with daily oral alitretinoin 30 mg or placebo for up to 24 weeks. Primary endpoint was proportion of responding patients based on Physician Global Assessment (PGA) of “clear” or “almost clear” at EOT. Key secondary endpoints: Patient Global Assessment (PaGA), change in modified Total Lesion Symptom Score (mTLSS), time to response (TTR), extent of disease at EOT, and duration of response (DOR). At EOT, 40% of alitretinoin-treated patients were responders vs 15% placebo-treated patients (odds ratio [OR] = 3.78; P < .001); a greater proportion of alitretinoin-treated patients achieved a PaGA of “cleared” or “almost cleared” (OR = 4.05; P< .001). A greater decrease in mTLSS occurred from baseline to EOT in alitretinoin- vs placebo-treated patients (treatment difference -24% P< .001). Median TTR for responders at EOT was shorter with alitretinoin vs placebo (65 vs 117 days; P< .001). Greater decreases in extent of disease at EOT were observed with alitretinoin vs placebo (treatment difference -22%; P< .001). The most common treatment-emergent adverse event was headache. Alitretinoin significantly improved signs/symptoms of sCHE, was well tolerated in patients refractory to potent topical corticosteroids, and may provide benefit to this population.
References:
-
- Bubna AK. Alitretinoin in Dermatology-An Update. Indian J Dermatol. 2015 Sep-Oct;60(5):520. doi: 10.4103/0019-5154.164426. PMID: 26538721; PMCID: PMC4601442.
- Panretin (alitretinoin) gel 0.1%. Panretin Package Insert. (n.d.). https://www.accessdata.fda.gov/drugsatfda_docs/label/1999/20886lbl.pdf
- Morganroth GS. Topical 0.1% Alitretinoin Gel for Classic Kaposi Sarcoma.Arch Dermatol. 2002;138(4):542–543. doi:10.1001/archderm.138.4.533
- Bodsworth NJ, Bloch M, Bower M, Donnell D, Yocum R; International Panretin Gel KS Study Group. Phase III vehicle-controlled, multi-centered study of topical alitretinoin gel 0.1% in cutaneous AIDS-related Kaposi’s sarcoma. Am J Clin Dermatol. 2001;2(2):77-87. doi: 10.2165/00128071-200102020-00004. PMID: 11705307.
- Fowler JF, Graff O, Hamedani AG. A phase 3, randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of alitretinoin (BAL4079) in the treatment of severe chronic hand eczema refractory to potent topical corticosteroid therapy. J Drugs Dermatol. 2014 Oct;13(10):1198-204. PMID: 25607554.
Featured Image Attribution
M. Sand, D. Sand, C. Thrandorf, V. Paech, P. Altmeyer, F. G. Bechara – M. Sand, D. Sand, C. Thrandorf, V. Paech, P. Altmeyer, F. G. Bechara: Cutaneous lesions of the nose. In: Head & face medicine Band 6, 2010, S. 7, ISSN 1746-160X. doi:10.1186/1746-160X-6-7. PMID 20525327. (Review). Open Access. CC BY 2.0
Did you enjoy this Therapeutic Cheat Sheet? You can find more here.