
Imaging is a mainstay of inpatient diagnostics. X-ray, MRI and CT scans are used to diagnose everything from broken bones to cancer. Yet these same imaging modalities are often ordered by hospitalists to diagnose dermatologic conditions even though the findings aren’t typically helpful in making an accurate diagnosis. These unnecessary tests are costly, delay an accurate diagnosis, and can add extra days to a hospitalization.
A scientific poster presented at the ODAC conference titled “The Impact of Imaging on Diagnostic Discordance in Inpatient Dermatology” evaluated the role imaging plays in the discordance between a hospitalist’s diagnosis and a dermatologist’s diagnosis. I interviewed poster author Shiv Patel, BA, of the University of Florida College of Medicine.
Inpatient dermatology imaging doesn’t get a lot of attention in dermatologic research. What led to your study?
In the inpatient setting, there is often an overreliance on imaging, and in some cases unnecessary imaging for dermatologic conditions. Non-dermatologists are more likely to use the imaging report findings when reaching a diagnosis rather than skin morphology, even though imaging findings are frequently non-specific. This dynamic can lead to increased costs, diagnostic delays, and potential mismanagement. Our study was motivated by a desire to better characterize how imaging is being used in inpatient dermatology and to highlight opportunities where dermatologic expertise can add the most value to patient care.
What’s the current state of inpatient dermatology in most hospitals? Which provider is most often requesting images and when in the process is the dermatology service involved?
In most hospitals, imaging for dermatologic conditions is commonly ordered by non-dermatology services, most often primary care, rather than by dermatologists themselves. The timing of dermatology consultations varies widely. In some cases, dermatology is consulted shortly after a rash is identified. On the other hand, dermatology may be consulted much later in the hospital course.
What are some of the repercussions of this framework?
Prior studies have demonstrated diagnostic discordance between primary care providers and dermatologists, underscoring the challenges of accurately diagnosing skin conditions. Therefore, when dermatologic diagnoses are delayed or incorrect, patients may experience inappropriate or unnecessary treatments, prolonged symptoms, and delays in initiating the correct therapy. As a result, this can lead to higher healthcare costs, longer hospital stays, and potentially progression of the underlying disease.
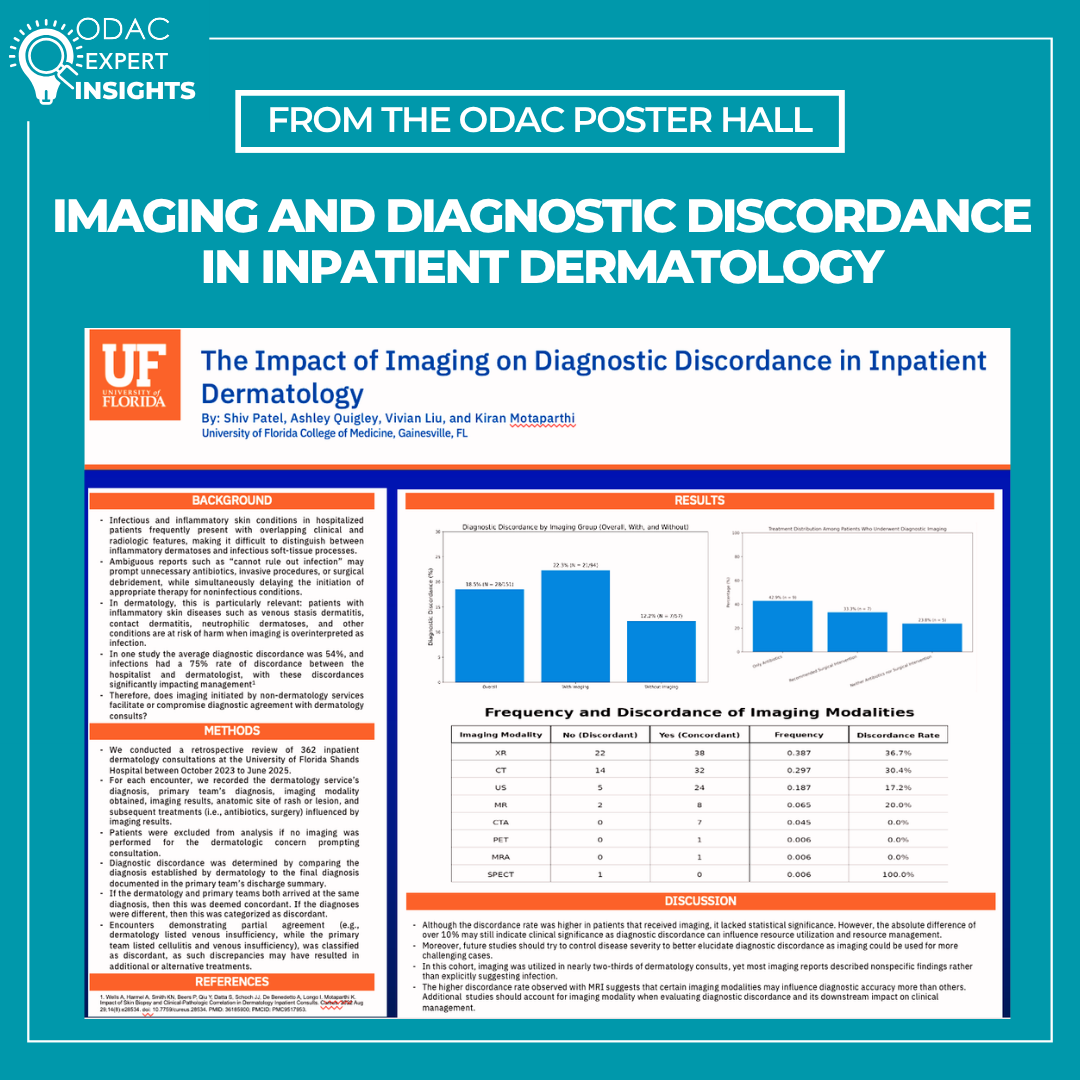
You conducted a review of inpatient dermatology consultations with imaging at UF Health Shands, looking at the rate of discordance between the hospitalist’s diagnosis and the dermatology service’s diagnosis. What did you discover? How did diagnostic discordance vary between imaging modalities?
Although the discordance rate was higher in patients that received imaging, it lacked statistical significance. However, the absolute difference of over 10% may still indicate clinical significance as diagnostic discordance can influence resource utilization and clinical management. We also observed variation in diagnostic discordance across different imaging modalities. However, because imaging modalities were not used in equal proportions, future studies should aim to normalize modality utilization to better elucidate the impact of specific imaging types on diagnostic discordance.
What needs to change in order to provide improved and efficient dermatology care to inpatients?
Improving inpatient dermatology care requires earlier and more consistent involvement of dermatology services. Greater emphasis on morphologic assessment and bedside evaluation, rather than reflexive imaging, can help streamline diagnosis and management. Lastly, clearer consultation pathways may reduce unnecessary testing and ultimately improve patient outcomes.
What else should dermatology clinicians know about this issue?
Dermatology clinicians should be aware that imaging is often obtained early in the inpatient course, frequently before dermatology is consulted, and may influence downstream diagnostic thinking despite its limited specificity for many skin conditions. This underscores the importance of early dermatologic involvement and clear communication with primary teams regarding the value of morphologic assessment. Dermatologists can also play a key role in educating inpatient teams about when imaging is unlikely to add diagnostic value and in advocating for more efficient, skin-directed diagnostic approaches.
Additional authors of the poster include:
Ashley Quigley, BS, University of Florida College of Medicine
Vivian Liu, MD, University of Florida College of Medicine
Kiran Motaparthi, MD, FAAD, University of Florida College of Medicine
Did you enjoy this scientific poster interview? You can find more here.