
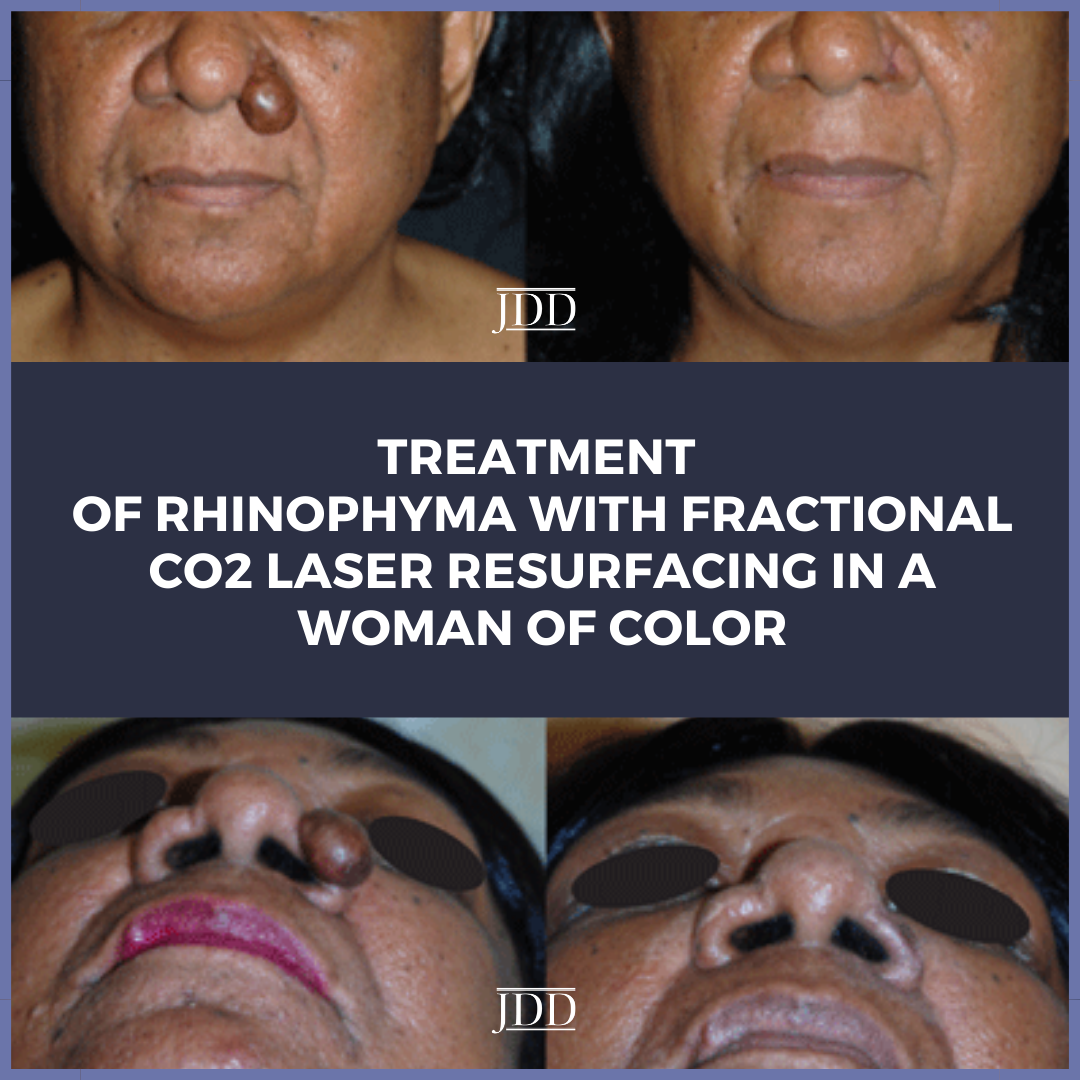
JDD authors Samuel S. Kassirer BA, Robert H. Gotkin MD, and Deborah S. Sarnoff MD present the first reported case of rhinophyma in a 62-year-old Fitzpatrick V female patient who was successfully treated with one session of fractional CO2 laser resurfacing. This case highlights the successful use of the fractional CO2 laser to treat rhinophyma in darker skin types (Fitzpatrick IV–VI) and underscores the potential for future use among patients of color.
Introduction
Rhinophyma, considered the culmination and most severe manifestation of acne rosacea, is a chronic, disfiguring dermatological disorder that may result in adverse psychological, functional, and cosmetic issues.1,2 The presentation of this phymatous subtype of rosacea is typically characterized by nodular hypertrophy of the alae and nasal tip, inflammation, telangiectasias, and erythema.3 Other forms of phymatous rosacea include gnathophyma, otophyma, blepharophyma, and metophyma.2 Although the pathogenesis is not fully understood, Demodex folliculorum, androgenic influence, vitamin deficiency, and vasodilator stimuli are thought to be contributing factors to the progression of rhinophyma.2,4-7 The pathologic process and the histopathology, however, are well described.8-10
Although acne rosacea is more prevalent among women (3:1), rhinophyma is more commonly found among men (20:1).1,2,11-13 Similarly, a significant discrepancy in the occurrence of rhinophyma exists between darker skin types (Fitzpatrick IV–VI) and lighter skin types (Fitzpatrick I–III), with reported cases among Fitzpatrick V–VI being exceptionally uncommon.2,10,14-16 We present a case of a 62-year-old Fitzpatrick V woman with a case of rhinophyma (Figure 1) who was successfully treated with fractional CO2 laser resurfacing of the nose. This rare case demonstrates the efficacy of fractional CO2 lasers to safely treat rhinophyma in patients of color, while improving their health, well-being, and cosmetic appearance.
Case Report

 A 62-year-old female patient of color (Fitzpatrick V) presented to one of the authors (DSS) for evaluation of an exophytic lesion on the left nasal ala that had gradually enlarged over the previous five years (Figure 1). The patient complained of difficulty with airflow through the left nostril as well as an increase in the swelling and size of the alar lesion and the nasal pores and an increase in sebum production of both paranasal regions. The patient sought medical attention due to psychological distress and self-consciousness regarding the appearance of the alar lesion. Pertinent history revealed that the patient described a warm central facial sensation that frequently occurred while she was cooking or when she was in the sun. She also noted that her face had become “more sensitive” over the recent past and stated that she was unable to tolerate many facial moisturizers due to stinging and burning sensations on her face. She denied the use of alcohol or other vasodilating stimuli.
A 62-year-old female patient of color (Fitzpatrick V) presented to one of the authors (DSS) for evaluation of an exophytic lesion on the left nasal ala that had gradually enlarged over the previous five years (Figure 1). The patient complained of difficulty with airflow through the left nostril as well as an increase in the swelling and size of the alar lesion and the nasal pores and an increase in sebum production of both paranasal regions. The patient sought medical attention due to psychological distress and self-consciousness regarding the appearance of the alar lesion. Pertinent history revealed that the patient described a warm central facial sensation that frequently occurred while she was cooking or when she was in the sun. She also noted that her face had become “more sensitive” over the recent past and stated that she was unable to tolerate many facial moisturizers due to stinging and burning sensations on her face. She denied the use of alcohol or other vasodilating stimuli.
Upon clinical examination, the patient showed signs of thickened skin across the entire lower half of the nose, a prominent exophytic lesion of the left ala and, with gentle pressure, sebum would emanate from the pores. The patient was also noted to have extensive dermatosis papulosa nigra on the face and trunk. All past medical history and medications were deemed unrelated and noncontributory.
A shave biopsy was performed to rule out cutaneous
malignancy as rhinophyma is known to mask nonmelanoma skin cancers. No skin cancer was found, and the histopathology report corroborated the initial diagnosis of rhinophyma; it outlined the presence of infundibular cysts, patchy lymphoplasmacytic infiltrates, and fibroplasia. Based on the previous successful treatment of patients with rhinophyma, both in the literature as well as with personal clinical experience, the use of fractional CO2 laser treatment was deemed appropriate and advised.14,17-19
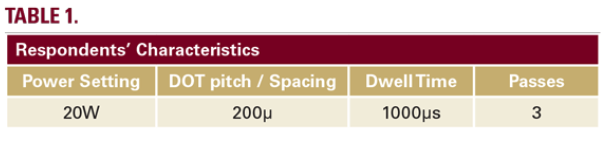
A loop cautery was employed to de-bulk and excise the exophytic lesion on the left ala. The patient then underwent a single treatment of fractional CO2 laser resurfacing. The DEKA SmartXide DOT fractional CO2 laser (DEKA, M.E.L.A., Calenzano, Italy) was used to fine-tune, contour and re-shape the left ala. The laser settings are noted in Table 1. The treated area was allowed to heal by secondary intention with frequent cleansing and the application of topical Aquaphor healing ointment and oral doxycycline twice a day for two weeks. The healing process was uneventful, and the patient reported both significant functional improvement, as well as aesthetic satisfaction, resulting in a return of positive self-esteem. One month after re-epithelialization, the patient showed signs of post-inflammatory hyperpigmentation; she was treated with topical 4% hydroquinone and 0.2% hydrocortisone valerate and was advised to apply a judicious amount of SPF 50+ zinc oxide sunblock daily. In addition, she was started on a once daily topical regimen of 1% ivermectin cream to control her inflammatory rosacea.
 Discussion
Discussion
Because rhinophyma can have profoundly negative psychosocial implications, both functional and aesthetic complications, as well as mask occult malignancies, a treatment that effectively addresses all of these concerns is necessary. The importance of early detection and early intervention in the treatment of rosacea are important steps in the prevention of rhinophyma and subsequent psychosocial, functional, and aesthetic complications associated with the deformity. This also includes dyspigmentation, which can be especially prominent in patients of color.17
The gradual progression from rosacea — a multiphasic cutaneous vascular condition — to rhinophyma follows an unvarying fourstage clinical course.1,5,8 The first stage, pre-rosacea, typically begins at the age of 30 to 60 years and is characterized by recurrent facial flushing.1,2 The increased blood flow to the superficial dermis results in the accumulation of excess extracellular fluid and the ensuing damage to the cutaneous facial lymphatic vessels promotes inflammatory edema.5 Consequently, transient erythema and early telangiectasias become apparent in the following stage, the vascular stage of rosacea. Erythema and telangiectasias can prove to be more difficult to detect in shades of skin with increased melanin, and this may obscure the clinician’s ability to accurately diagnose rosacea in a timely fashion. Reported incidences of both rosacea and rhinophyma are less common in darker skin types; this highlights the importance of this case.14,17,18
In the inflammatory stage, the third stage of rosacea, telangiectasias increase and pustules and papules develop into acne rosacea.1,2,5,8 In the late stage, inflammation continues to increase and fibroplasia and sebaceous gland hyperplasia of the nasal skin produce hypertrophy and thickening of the dermis of the caudal nose; this results in the well-known clinical manifestations of rhinophyma.9 Inspissated sebum and bacteria can become trapped in the dilated sebaceous pores, plugging the cystic sebaceous ducts and chronically infecting the nasal skin.2 Pits, fissures, and scarring of the enlarged nasal tip distort and disfigure the shape and contour of the nose. The resulting deformity can be both cosmetic and functional as secondary nasal airway obstruction may occur.10,11 The subsequent respiratory issues, difficulty eating and drinking, and the psychological distress that can accompany rhinophyma necessitate treatment that addresses all of the functional and cosmetic issues.2,8,10,11
Treatment of rhinophyma is dependent on a multitude of factors, including its severity, the patient’s skin type, and the simultaneous presence of malignant tissue.2,7,11,12 Treatments that have proven to be effective in curtailing various stages of rosacea in both patients with darker skin (Fitzpatrick IV– VI) and lighter skin types (Fitzpatrick I–III) include avoidance of predisposing factors, antibiotic therapy, isotretinoin and other retinoids, anti-inflammatory medication, and use of other agents that decrease flushing.1,2,5,7,11,18 Non-surgical therapies, however, are inadequate to treat well-established rhinophyma.7,11 Effective treatment options include total excision, partial excision or decortication, and laser excision. The various methods available are full-thickness excision with skin graft or flap reconstruction; dermaplaning; dermabrasion; cryotherapy; radiotherapy; chemical peel; electrocautery; cold or heated scalpel excision; and Nd:YAG, argon, Er:YAG, and CO2lasers.7,11,13,20-23 Potential non-surgical treatments, like tamoxifen, which targets increased fibroblast function in rhinophyma through down-regulation of TGF-β, are currently undergoing research.1,2,9,19
Although there are a variety of surgical and laser treatments available, treatment of rhinophyma using CO2 lasers has proven to be a very effective method with exceptional cosmetic results that often surpass the traditional surgical techniques.7,11,14,20-23 The fractional CO2 laser emits light at a wavelength of 10,600nm; this laser energy is heavily absorbed by intracellular and extracellular water.12 Fractional CO2 lasers deliver light in distinct columns termed microscopic thermal treatment zones —
columns of ablation surrounded by intact tissue. Through vaporization by laser-generated heat, tissue is removed and collagen is regenerated during the wound-healing phase; this results in the reorganization of the epidermis and dermis during the process of neocollagenesis.14 When compared with other treatment methods, treatment using fractional CO2 lasers has been shown to have a bloodless surgical field with no blood loss, precise contouring, simple post-operative care, rapid healing and shorter patient downtime, low scarring risk, and predictably good cosmetic results. Disadvantages include expensive equipment, accentuation of pores, and transient pigmentary alterations.7,11,13
The successful use of CO2 lasers to treat rhinophyma is well documented and has been reported previously in patients with lighter skin types.7,11,13, 20-23 To the best of our knowledge, this is the first reported case of fractional CO2 laser resurfacing used to treat rhinophyma in a female patient of color (Fitzpatrick V). There has been one reported case on the successful use of a fractional CO2 laser resurfacing to treat mild rhinophyma in a male patient of color (Fitzpatrick VI).14Likewise, success in this case further demonstrates the efficacy of fractional CO2 lasers in the treatment of well-developed cases of rhinophyma in patients with darker skin types (Fitzpatrick IV–VI). Although there was the expected post-inflammatory hyperpigmentation, the use of topical hydroquinone, steroid, and SPF 50+ zinc oxide sunblock resolved this issue in a timely manner.
There is a misperception that people of color do not develop rosacea. Compared to Fitzpatrick I–III skin types, the difficulty detecting erythema and telangiectasias in darker skin may lead to its under-diagnosis. Many people with skin of color who have rosacea might experience delayed diagnosis; this could potentially lead to progressive disease with disfiguring manifestations including phymatous rosacea.24
Conclusion
Disclosures
Acknowledgement
References
2. Rohrich RJ, Griffin JR, Adams WP. Rhinophyma: Review and update. Plast Reconstr Surg. 2002;110(3):860-870.
3. Classification of rosacea. https://www.rosacea.org/physicians/classificationof- rosacea/view-online. Accessed April 2, 2021.
4. Roihu T, Kariniemi A-L. Demodex mites in acne rosacea. J Cutan Pathol. 1998;25(10):550-552.
5. Wilkin JK. Rosacea. Arch Dermatol. 1994;130(3):359.
6. Popa D, Osman G, Parvanescu H, et al. The treatment of giant rhinophyma – Case Report. Curr Health Sci J. 2012;38(1):41-44.
7. Simo R, Sharma V. The use of the CO2 laser in rhinophyma surgery: Personal technique and experience, complications, and long-term results. Facial Plastic Surgery. 1998;14(04):287-295.
8. Cohen AF, Tiemstra JD. Diagnosis and treatment of rosacea.J Am Board Fam Pract. 2002;15(3):214-217.
9. Schüürmann M, Wetzig T, Wickenhauser C, et al. Histopathology of rhinophyma: A clinical-histopathologic correlation. J Cutan Pathol. 2015;42(8):527-535.
10. Marks R. Concepts in the pathogenesis of rosacea. Br J Dermatol. 1968;80(3):170-177.
11. Little S, Stucker F, Compton A, et al. Nuances in the management of rhinophyma. Facial Plast Surg. 2012;28(02):231-237.
12. Moreira A, Leite I, Guedes R, et al. Surgical treatment of rhinophyma using carbon dioxide (CO2) laser and pulsed dye laser (PDL). J Costmet Laser Ther. 2010;12(2):73-76.
13. Bogetti P, Boltri M, Spagnoli G, et al. Surgical treatment of rhinophyma: A comparison of techniques. Aesthet Plast Surg. 2002;26(1):57-60.
14. Kraeva E, Ho D, Jagdeo J. Successful treatment of rhinophyma with fractionated carbon dioxide (CO2) laser in an African-American man: Case report and review of literature of fractionated CO2 laser treatment of rhinophyma. J Drugs Dermatol. 2016;15(11):1465-1468.
15. Wollina U, Verma SB. Rosacea and rhinophyma: not curse of the Celts but Indo Eurasians. J Cosmet Dermatol. 2009;8(3):234-235.
16. Allah KC, Kossoko H, Yéo S, et al. Rhinophyma chez un noir. Revue de Stomatologie et de Chirurgie Maxillo-faciale.2009;110(6):347-349
17. Rosacea Found in African Americans. Rosacea Found in African Americans / Rosacea.org. https://www.rosacea.org/rosacea-review/1997/winter/rosaceafound- in-african-americans. Accessed April 2, 2021.
18. Browning DJ, Rosenwasser G, Lugo M. Ocular rosacea in Blacks. Am J Opthalmol. 1986;101(4):441-444.
19. Payne WG, Ko F, Anspaugh S, et al. Down-regulating causes of fibrosis with tamoxifen. Ann Plast Surg. 2006;56(3):301-305.
20. Kassir R, Gilbreath J, Sajjadian A. Combination surgical excision and fractional carbon dioxide laser for treatment of rhinophyma. World J Plast Surg. 2012;1(1):36-40.
21. Meesters AA, van der Linden MM, De Rie MA, et al. Fractionated carbon dioxide laser therapy as treatment of mild rhinophyma: Report of three cases. Dermatol Ther. 2015;28(3):147-150.
22. Serowka KL, Saedi N, Dover JS, et al. Fractionated ablative carbon dioxide laser for the treatment of rhinophyma. Lasers Surg Med. 2013;46(1):8-12.
23. Krausz AE, Goldberg DJ, Ciocon DH, Tinklepaugh AJ. Procedural management of rhinophyma: A comprehensive review. J Cosmet Dermatol. 2018; 6:960-967.
24. Alexis AF, Callender VD, Baldwin HE, Desai SR, Rendon MI, Taylor SC. Global epidemiology and clinical spectrum of rosaea, highlighting skin of color: Review and clinical practice experience. J Am Acad Dermatol. 2019 Jun; 80(6):1722-1729.e7, accessed 2/23/2021.
Source
Kassirer S. S., Gotkin H., Sarnoff D. S. Treatment of Rhinophyma With Fractional CO2 Laser Resurfacing in a Woman of Color: Case Report and Review of the Literature. Journal of drugs in dermatology: JDD, 20(7). Published early online June 23 2021.
Content and images used with permission from the Journal of Drugs in Dermatology.
Adapted from original article for length and style.
Did you enjoy this JDD Case Report? You can find more here.