

Generalized pustular psoriasis (GPP) is a rare, autoinflammatory condition, with acute, severe flares of diffuse sterile pustules and systemic symptoms that can be life-threatening. Historically, cyclosporine, methotrexate, retinoids, and biologics modulating the interleukin-17 (IL-17), IL-23, and tumor necrosis factor α pathways have been used off-label for management.1 Aberrant IL-36 signaling has been implicated in subsets of patients with GPP.2 We continue our series, Therapeutic Cheat Sheet, with a closer look at spesolimab, the only FDA-approved medication to date for treating generalized pustular psoriasis, now with new subcutaneous dosing! Because spesolimab is relatively new to market, evidence for off-label use is limited to case reports.
Spesolimab Therapeutic Cheat Sheet
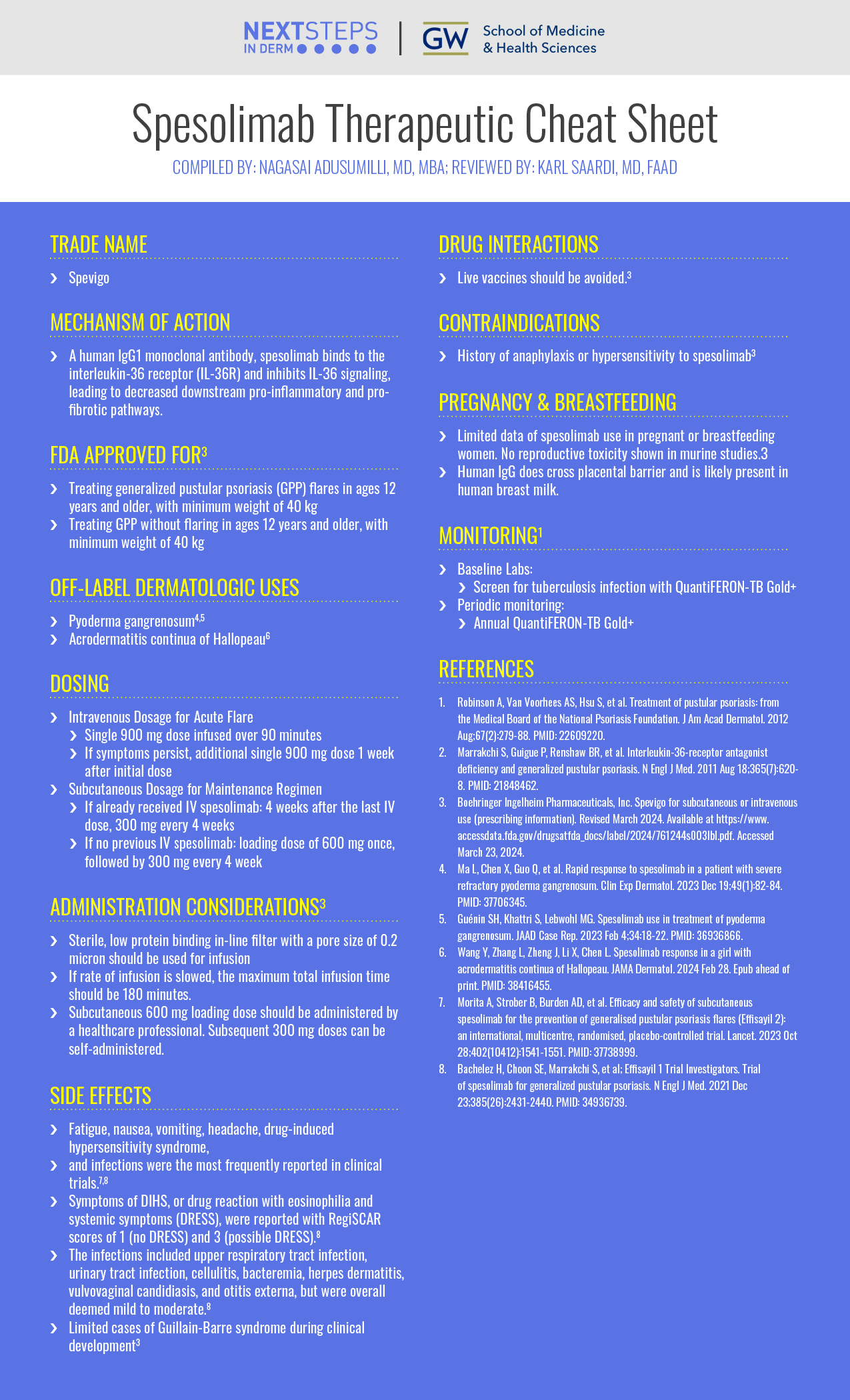
Compiled by: Nagasai Adusumilli, MD, MBA | Reviewed by: Karl Saardi, MD
TRADE NAME
-
- Spevigo
MECHANISM OF ACTION
-
- A human IgG1 monoclonal antibody, spesolimab binds to the interleukin-36 receptor (IL-36R) and inhibits IL-36 signaling, leading to decreased downstream pro-inflammatory and pro-fibrotic pathways.
FDA-APPROVED FOR3
-
- Treating generalized pustular psoriasis (GPP) flares in ages 12 years and older, with minimum weight of 40 kg
- Treating GPP without flaring in ages 12 years and older, with minimum weight of 40 kg
OFF-LABEL DERMATOLOGIC USES
-
- Pyoderma gangrenosum4,5
- Acrodermatitis continua of Hallopeau6
DOSING3
Intravenous Dosage for Acute Flare
-
- Single 900 mg dose infused over 90 minutes
- If symptoms persist, additional single 900 mg dose 1 week after initial dose
Subcutaneous Dosage for Maintenance Regimen
-
- If already received IV spesolimab: 4 weeks after the last IV dose, 300 mg every 4 weeks
- If no previous IV spesolimab: loading dose of 600 mg once, followed by 300 mg every 4 weeks
ADMINISTRATION CONSIDERATIONS3
-
- Sterile, low protein binding in-line filter with a pore size of 0.2 micron should be used for infusion
- If rate of infusion is slowed, the maximum total infusion time should be 180 minutes.
- Subcutaneous 600 mg loading dose should be administered by a healthcare professional. Subsequent 300 mg doses can be self-administered.
SIDE EFFECTS
-
- Fatigue, nausea, vomiting, headache, drug-induced hypersensitivity syndrome, and infections were the most frequently reported in clinical trials.7,8
- Symptoms of DIHS, or drug reaction with eosinophilia and systemic symptoms (DRESS), were reported with RegiSCAR scores of 1 (no DRESS) and 3 (possible DRESS).8
- The infections included upper respiratory tract infection, urinary tract infection, cellulitis, bacteremia, herpes dermatitis, vulvovaginal candidiasis, and otitis externa, but were overall deemed mild to moderate.8
- Limited cases of Guillain-Barre syndrome during clinical development3
DRUG INTERACTIONS
-
- Live vaccines should be avoided.3
CONTRAINDICATIONS
-
- History of anaphylaxis or hypersensitivity to spesolimab3
PREGNANCY AND BREASTFEEDING
-
- Limited data of spesolimab use in pregnant or breastfeeding women. No reproductive toxicity shown in murine studies.3
- Human IgG does cross placental barrier and is likely present in human breast milk.
MONITORING
-
- Baseline Labs:
- Screen for tuberculosis infection with QuantiFERON-TB Gold+
- Periodic monitoring:
- Annual QuantiFERON-TB Gold+
- Baseline Labs:
REFERENCES
-
- Robinson A, Van Voorhees AS, Hsu S, et al. Treatment of pustular psoriasis: from the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2012 Aug;67(2):279-88. PMID: 22609220.
- Marrakchi S, Guigue P, Renshaw BR, et al. Interleukin-36-receptor antagonist deficiency and generalized pustular psoriasis. N Engl J Med. 2011 Aug 18;365(7):620-8. PMID: 21848462.
- Boehringer Ingelheim Pharmaceuticals, Inc. Spevigo for subcutaneous or intravenous use (prescribing information). Revised March 2024. Available at https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/761244s003lbl.pdf. Accessed March 23, 2024.
- Ma L, Chen X, Guo Q, et al. Rapid response to spesolimab in a patient with severe refractory pyoderma gangrenosum. Clin Exp Dermatol. 2023 Dec 19;49(1):82-84. PMID: 37706345.
- Guénin SH, Khattri S, Lebwohl MG. Spesolimab use in treatment of pyoderma gangrenosum. JAAD Case Rep. 2023 Feb 4;34:18-22. PMID: 36936866.
- Wang Y, Zhang L, Zheng J, Li X, Chen L. Spesolimab response in a girl with acrodermatitis continua of Hallopeau. JAMA Dermatol. 2024 Feb 28. Epub ahead of print. PMID: 38416455.
- Morita A, Strober B, Burden AD, et al. Efficacy and safety of subcutaneous spesolimab for the prevention of generalised pustular psoriasis flares (Effisayil 2): an international, multicentre, randomised, placebo-controlled trial. Lancet. 2023 Oct 28;402(10412):1541-1551. PMID: 37738999.
- Bachelez H, Choon SE, Marrakchi S, et al; Effisayil 1 Trial Investigators. Trial of spesolimab for generalized pustular psoriasis. N Engl J Med. 2021 Dec 23;385(26):2431-2440. PMID: 34936739.
Did you enjoy this Therapeutic Cheat Sheet? You can find more here.