Learn more about what it’s like to be a dermatologist today and what it takes to transition from residency to being a practicing dermatologist.
Find hands-on clinical pearls to help you care for your patients more effectively, stay up-to-date with the latest research, or stop by often for expert advice from industry leaders and insights on what it takes to be a key opinion leader.
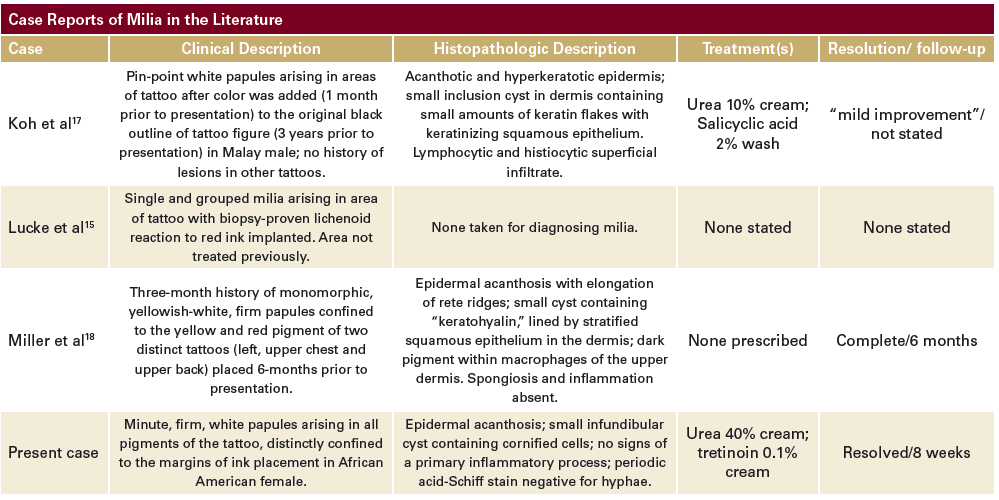
The most frequently reported tattoo-related dermatoses, according to a study of 234 tattooed patients, are allergic,1infectious,2,3 and granulomatous4,5 reactions occurring in 2.1% of this population.6 Less common reactions are lichenoid,7photoallergic,8 pseudolymphomatous,9 discoid lupus erythematosus,10 incidental skin neoplasm,11 and koebnerization of psoriasis.12,13Milia within tattoos are rare, with only three reports in the English literature (Table 1). This case is used to illustrate relevant findings, discuss the proposed pathogenesis and review treatment options.
Case Report
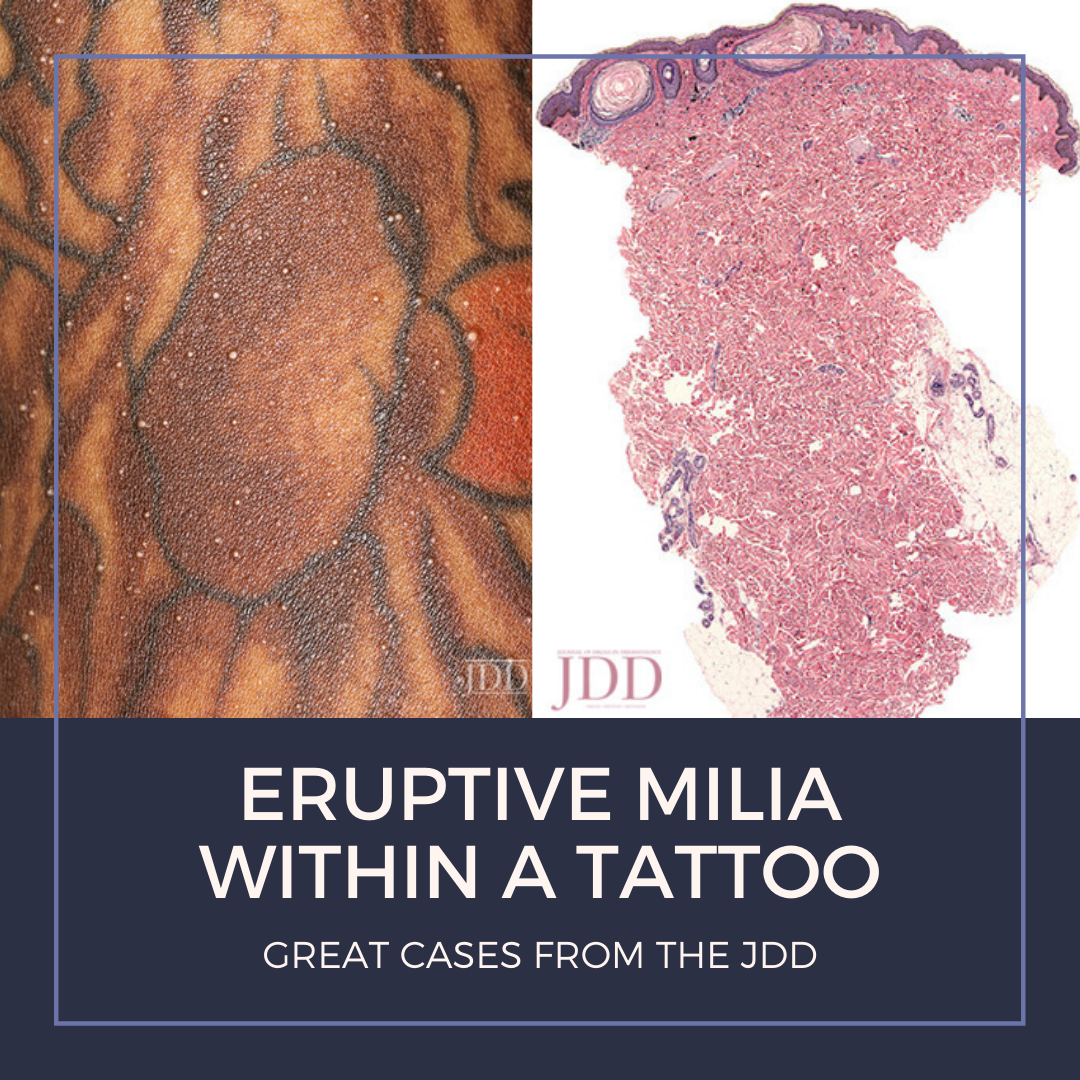
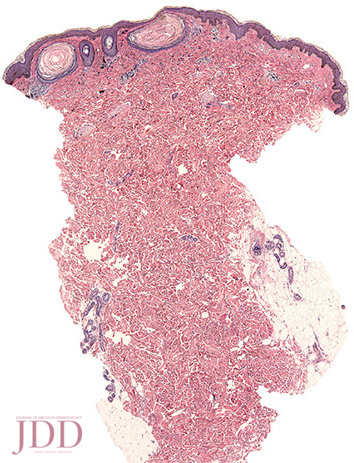
A 19-year-old African American female with no past medical history presented with new white papules arising within a tattoo on the left upper chest, shoulder, and arm. Lesions appeared one month after tattoo placement, which was inked six months prior to presentation. Prior to the visit, the patient had tried over the counter antibiotic ointment with no improvement. She denied pruritus, pain, bleeding, or other symptoms. Aside from tattoo placement, there was no trauma to the site. She denied use of other topical or systemic medications. On physical examination, there were multiple, minute, firm, monomorphic, white papules arising within various pigments of the tattoo (Figure 1). Lesions were confined within the margins of the tattoo, sparing adjacent skin (Figure 2). Similar findings were absent from her other tattoos. A punch biopsy of a lesion on the left shoulder demonstrated deposits of black granular material in the dermis and small, infundibular cysts containing cornified cells (Figures 3 and 4). There were no signs of a primary inflammatory process. Periodic Acid-Schiff stain was negative for hyphae (Figures 3 to 5). Daily urea 40% cream was prescribed with significant reduction in size and number of milia. Upon follow-up, her treatment regimen was supplemented with tretinoin 0.1% cream.
Table 1
FIGURE 1. Milia within red, orange, green, brown and black pigments of a tattoo. Note: sparing of non-inked skin.
FIGURE 2. Magnified view of milia confined within the margins of a tattoo.
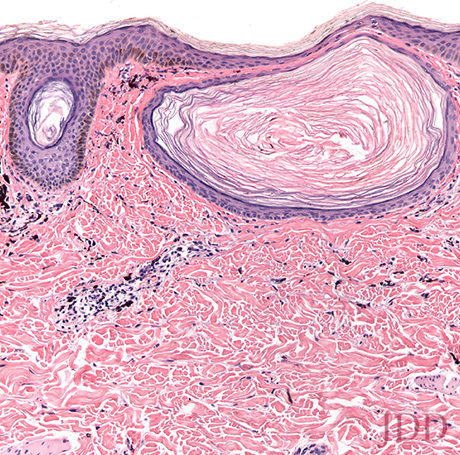
FIGURE 3. Dark granules of pigment intra- and extra-cellularly and small cysts containing lamellar keratin (Hematoxylin & Eosin, origi-nal magnification x 40).
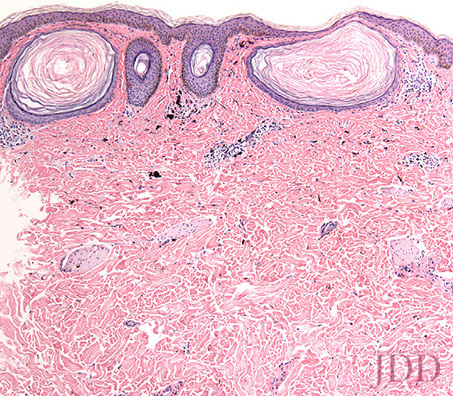
FIGURE 4. Dermal cysts containing lamellar keratin within the follicu-lar infundibulum (Hematoxylin & Eosin, original magnification x100).
FIGURE 5. Dermal cysts; note that two within follicular infundibula, containing lamellar keratin (Hematoxylin & Eosin, original magnifica-tion x200).
Discussion
Tattoos serve both religious and aesthetic decorative purposes. Previously, tattoos were associated with regimented and marginalized groups, however, increasing popularity over the last two decades has made them mainstream.14Clinically, milia within tattoos present as small, yellowish papules within tattoo pigments. There is no accompanying history of trauma and the lesions can appear at any time following inking. While the condition can be pruritic, patients are mostly asymptomatic and typically present weeks-to-months following placement of the tattoo. However, milia have also even been reported within a longstanding tattoo, appearing in the setting of a lichenoid reaction to red ink.15Histopathologically, milia in tattoos are characterized by small keratinized cysts lined by stratified squamous epithelium with keratin arranged in concentric lamellae.16 Pigment is found within macrophages and extracellularly in the dermis. Inflammation and spongiosis are absent. The pathogenesis of eruptive milia is incompletely understood, although it is most likely due to trauma. Generally, milia are categorized as primary or secondary. Primary lesions arise from pilosebaceous units of vellus hair follicles. Secondary milia result from trauma or bullous and inflammatory disorders.16 The authors suggest that needling used for ink placement results in traumatic implantation of the epidermis into the dermis; the process also disrupts adnexal structures. Additionally, application of a tattoo produces an acute, aseptic inflammatory reaction. A prior report of milia within a lichenoid tattoo reaction showed disruption of adnexal structures on histology.15 This trauma, therefore, is akin to that of secondary milia formation. Moreover, post-tattoo care regimens, such as ointment massage and occlusion, may increase accumulation of keratin debris within the needle wounds and follicular ostia. Although this may further follicular obstruction and milia formation, there are likely other factors involved, as these care regimens would likely affect normal adjacent skin. While the condition is benign and self-limited, patients often request therapy secondary to aesthetic concerns. In cases with few lesions, a needle or scalpel can be used to express individual cysts. Keratolytics, such as tretinoin, urea, and salicylic acid, have been used to reduce ostial plugging by normalizing epidermal maturation. They hasten resolution through exfoliation. Non-ablative and ablative lasers can also improve milia within tattoos, but are likely to disrupt the design clarity and pigment, making this a less favorable treatment.In summary, this case of eruptive milia in a tattoo demonstrates an exceedingly rare complication of skin-inking. It is important for clinicians to be able to distinguish this reaction from others that likely require more aggressive therapy. As tattooing is a trend on the rise, dermatologists can expect to see an increased number of tattoo-related dermatoses in their practice.14
References
Ravits H. Allergic Tattoo Granuloma. Arch Dermatol. 1962;86(3):287-289.
Kluger N, Cohen P, Fallet-Bianco C, Guillevin L. Mycobacterium chelonae infection under adalimumab therapy for spondylarthritis. Clin Exp Rheumatol. 2010;28(1):101-102.
Samuel MC, Doherty PM, Bulterys M, Jenison SA. Association between heroin use, needle sharing and tattoos received in prison with hepatitis B and C positivity among street-recruited injecting drug users in New Mexico, USA. Epidemiol Infect. 2001;127(3):475-484.
Schwartz RA, Mathias CG, Miller CH, Rojas-Corona R, Lambert WC. Granulomatous reaction to purple tattoo pigment. Contact dermatitis. 1987;16(4):198-202.
Sowden JM, Cartwright PH, Smith AG, Hiley C, Slater DN. Sarcoidosis presenting with a granulomatous reaction confined to red tattoos. Clin Exp Dermatol. 1992;17(6):446-448.
Kazandjieva J, Tsankov N. Tattoos: dermatological complications. Clin Dermatol. 2007;25(4):375-382.
Sanghavi SA, Dongre AM, Khopkar US. Tattoo reactions–an epidemic on the surge: a report of 3 cases. Indian J Dermatol Venereol Leprol. 2013;79(2):231-234.
Bjornberg A. Reactions to Light in Yellow Tattoos from Cadmium Sulfide. Arch Dermatol. 1963;88:267-271.
Marchesi A, Parodi PC, Brioschi M, et al. Tattoo Ink-Related Cutaneous Pseudolymphoma: A Rare but Significant Complication. Case Report and Review of the Literature. Aesthetic Plast Surg. 2014;38:471.
La Placa M, Passarini B. Subacute cutaneous lupus erythematosus after a tattoo. Clin Exp Dermatol. 2009;34(5):632-633.
West CC, Morritt AN, Pedelty L, Lam DG. Cutaneous leiomyosarcoma arising in a tattoo – ‘a tumour with no humour’. J Plast Reconstr Aesthet Surg. 2009;62(5):e79-80.
Smith SF, Feldman SR. Tattoo sites and psoriasis. J Drugs Dermatol. 2011;10(10):1199-1200.
Horner KL, Chien AJ, Edenholm M, Hornung RL. Winnie the Pooh and psoriasis too: an isomorphic response of guttate psoriasis in a tattoo. Pediatr Dermatol. 2007;24(5):E70-72.
Juhas E, English JC, 3rd. Tattoo-associated complications. J Pediatr Adolesc Gynecol. 2013;26(2):125-129.
Lucke T, Fallowfield M, Burden D. Lichen planus associated with milia. Clin Exp Dermatol. 1999;24(4):266-269.
Epstein W, Kligman AM. The pathogenesis of milia and benign tumors of the skin. J Invest Dermatol. 1956;26(1):1-11.
Koh MJ, Teo RY, Liu TT. Multiple epidermal cysts occurring in a tattoo. Singapore Med J. 2009;50(11):e376-377.
Miller LM, Schwartz JT, Cho S. Milia: a unique reaction to tattoos. Cutis. 2011;87(4):195-196.
Source:
Nicholas Ross, Michele Farber MD, and Joya Sahu MD, (2017). Eruptive Milia Within a Tattoo: A Case Report and Review of the Literature. Journal of Drugs in Dermatology,16(6), 621-624.