
Okay, okay, okay, I didn’t actually use AI to write this article. But, like many people in today’s world, I have utilized AI to streamline things in both my personal and professional life.
No matter your personal feelings about AI, it is clear that it is now part of our world. Artificial intelligence (AI) is defined as the ability of a computer to perform tasks typically associated with humans, such as problem-solving, pattern recognition, and language use. The conceptual foundation for AI began in the mid-20th century with Alan Turing (who, as a reminder, was the British mathematician who cracked the Nazi Enigma code in World War II). Turing’s work on theoretical computing and the “Turing machine” helped establish the idea that machines could perform logical operations. Early AI programs followed in Turing’s wake and became a formal field of study in the 1950s and 60s. Progress wasn’t linear, however, with periods of rapid growth and optimism followed by “AI winters” when expectations outpaced available technology and public opinion soured.
AI advanced substantially with improvements in computing power, data availability, machine learning, and, later, deep learning (dammit, Jim, I’m a doctor, not a computer scientist! The internet says deep learning is the underlying method that allows computers to identify complex patterns in data). The important point is that these advances enabled computers to process language and generate human-like responses at a scale previously unattainable.
The release of ChatGPT by OpenAI on November 30, 2022, marked a major public turning point because it made generative AI (the use of deep learning engines to create new content) accessible through natural conversation rather than specialized software. Since then, AI models have quickly entered healthcare discussions with potential uses in many facets of the medical system. At the same time, AI has raised important concerns about accuracy, bias, privacy, and the need for clinician oversight. Beyond these clinical and ethical concerns, AI has also drawn criticism for its environmental impact. The substantial infrastructure required to support AI, including large data centers, consumes significant electricity and water for computing and cooling. As generative AI use expands, its environmental footprint should remain central to discussions about the responsible incorporation of AI into healthcare.
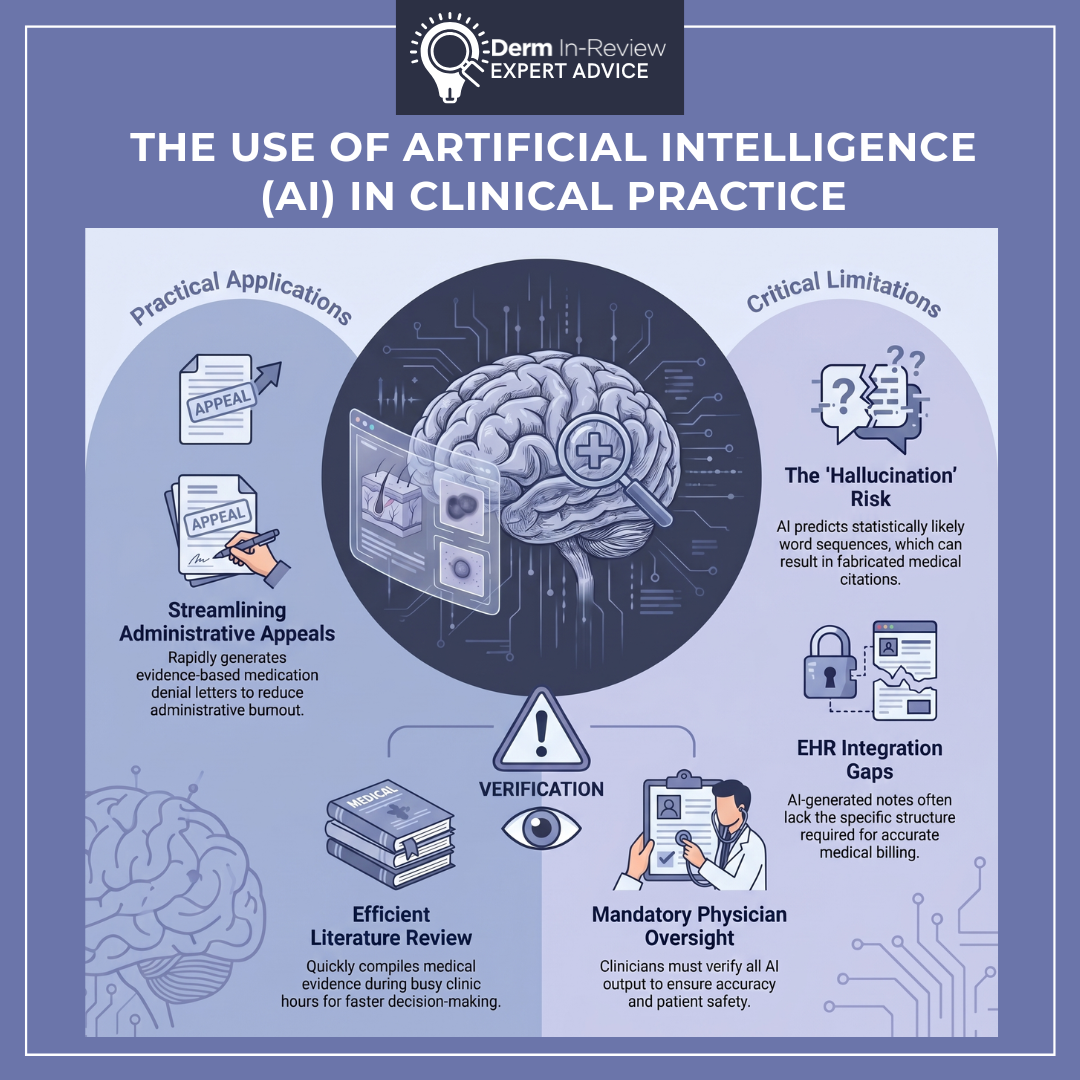
In my personal practice, and potentially in yours, AI currently has a limited but useful role. My institution has recently integrated an AI clinical agent into our EHR with, in my opinion, limited success so far. The concept makes a lot of sense: less time typing, better capture of the patient encounter, and more attention directed toward the patient rather than the computer. (Who doesn’t love the idea of not writing notes 24/7?) The reality, at least in its current form, has been much more mixed. AI-generated notes are often long and cumbersome, and they do not always translate the visit into a note structure that supports accurate coding. Sure, they may capture what was said with precise detail, but they often lack support for the medical decision-making that billing departments need to identify the appropriate level of service. I can see how this technology may become a game-changer moving forward, particularly as these tools become more specialty-specific and better integrated into clinical workflows, but we are not quite there yet. Personally, I am holding out for AI documentation that goes beyond summarizing the visit. I want tools that reduce click fatigue, suggest appropriate prescription orders, incorporate my own dot phrases, and understand the nuances of medical decision-making as it pertains to billing. These tools have all been promised, yet I’ll believe it when I see it.
By far, the most useful application of AI in my clinical practice has been the quick and painless creation of appeal letters for medication denials, which, as we all know too well, are happening with increasing frequency. For example, I may enter a prompt such as, “My patient is a 27-year-old female with psoriasis, BSA 15%, who has trialed and failed three months of topical corticosteroids. She is considering pregnancy in the near future. Insurance is requiring a trial of methotrexate prior to biologic coverage. Write me an appeal letter with citations of current evidence.” Generative AI can produce an often near-perfect appeal letter, which I then review, verify, and tailor with the appropriate patient-specific details. Key word here being verify. Large language models have been known to “hallucinate,” or produce information that sounds right, but is actually fabricated or incorrect, including things like made-up academic papers and fake book references. These errors are not a result of bad programming; they occur because these models predict what is most statistically likely to come next in a sequence of words. Even if the underlying information is missing, the model completes the pattern anyway. That’s why hallucinations appear when prompts demand certainty, or when the model is pushed to answer things beyond what its data can reliably support.
Finally, AI has the ability to rapidly evaluate and compile information, making literature review much more efficient. This can be particularly helpful when trying to quickly compile evidence during a busy clinic. The major limitation, of course, is accuracy. Interestingly, emerging comparative data suggest that the tools marketed most specifically for healthcare professionals may not always outperform generalist large language models. (In other words, ChatGPT performed superiorly to OpenEvidence and UpToDate Expert AI in ‘medical knowledge benchmark’ tests.) While this does not mean generalist AI is the superior tool in healthcare, it suggests AI tools vary substantially in quality, and even “medical” AI platforms require careful verification, source-checking, and physician oversight.
Ultimately, AI has about as many limitations as it does possibilities. It is a tool, and like any tool, its value depends on how thoughtfully we use it. For dermatologists, its most practical role right now may be helping us move faster through the administrative (and soul-sucking) parts of practice: drafting appeals, searching the literature, generating dot phrases, and reducing some of the burnout that competes with patient care. But we are still the experts, and it falls to us to make sure that we are using our tools responsibly. Used carefully, AI may give us back a little time and mental space (mandatory wellness exercise?). Used carelessly, it can create new problems under the illusion of efficiency. As with most things in medicine, the answer is probably somewhere in the land of gray.
Let me know if you want this shortened or expanded. If you’d like, I can also turn this into a PowerPoint outline, discussion post, or shorter summary.
….. (kidding again!)
References
– Vishwanath K, Ghosh M, Alyakin A, Alber DA, Aphinyanaphongs Y, Oermann EK. Generalist large language models outperform clinical tools on medical benchmarks. arXiv. Published December 1, 2025. doi:10.48550/arXiv.2512.01191
– Edward G. Poon, Christopher H. Lemak, Juan C. Rojas, John Guptill, David Classen. Adoption of artificial intelligence in healthcare: survey of health system priorities, successes, and challenges. J Am Med Inform Assoc. 2025;32(7):1093-1100. doi:10.1093/jamia/ocaf065. PMID:40323320; PMCID:PMC12202002. Available from: PMC article
– The Editors of Encyclopaedia Britannica. Encyclopaedia Britannica. History of artificial intelligence. In: Encyclopaedia Britannica. Updated 2025. Accessed May 20, 2026. Available from: Britannica article
– Tableau AI history article. History of AI: From beginnings to modern applications. Published 2024. Accessed May 20, 2026.