
Prurigo nodularis (PN) is far more than just a persistent itch—it is a distinct, neuroimmune-driven disease entity that demands its own targeted diagnostic and therapeutic roadmap. During a standout session at this year’s Skin of Color Update in New York City, Dr. Raj Chovatiya challenged the long-held notion that PN is merely a variant of atopic dermatitis. For patients with skin of color, where dyspigmentation and the relentless itch-scratch cycle carry an immense psychosocial burden, Dr. Chovatiya argued that understanding this biological distinction is the first critical step toward providing truly effective, patient-centered care.
Understanding Prurigo Nodularis
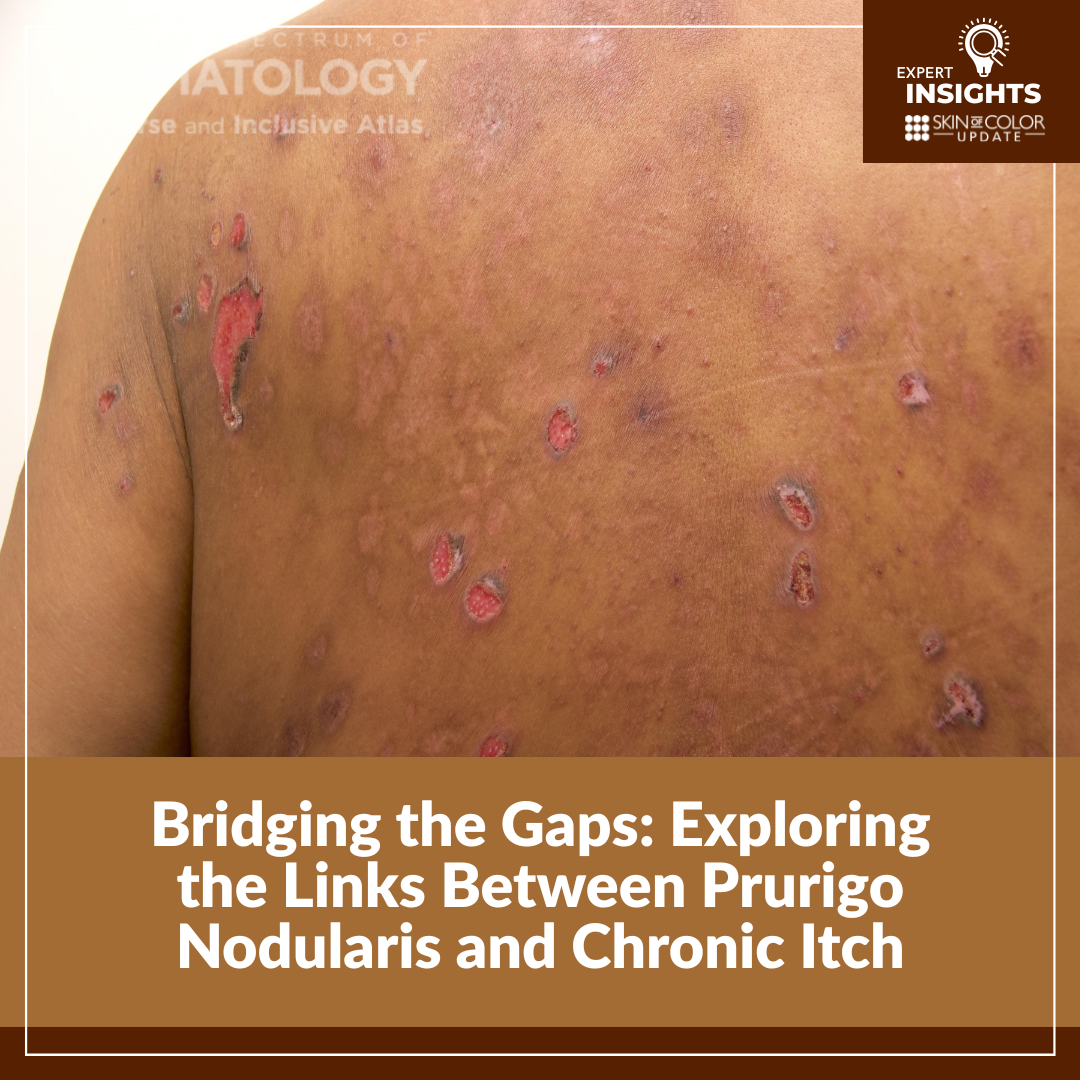
First described by Hyde in 1909, PN is characterized by symmetric and bilaterally distributed hyperkeratotic nodules accompanied by intense, chronic, intractable pruritus. Dr. Chovatiya emphasized that PN’s clinical presentation can be highly variable, with nodules, papules, plaques, erosions, or scarring. Lesions may number from a handful to hundreds, and secondary changes such as excoriation, lichenification, xerosis, and pigment alteration are especially pronounced in patients with skin of color, where dyspigmentation can persist even after inflammation resolves. The itch-scratch cycle in PN is relentless, and even when lesions heal, pigmentary changes can be long-lasting, adding an additional psychosocial burden for patients with darkly pigmented skin.
PN remains a clinical diagnosis, supported by three key diagnostic criteria: (1) Firm papulonodular lesions, (2) Chronic pruritus lasting more than six weeks, and (3) A history of scratching, rubbing, or picking. Dr. Chovatiya underscored the importance of a thorough history and physical examination as the cornerstone of diagnosis. Laboratory testing such as CBC, CMP, thyroid and iron studies may help rule out systemic contributors, but clinicians should not delay therapy while awaiting results.
The Burden of Itch
In PN, itch is not merely a symptom; it is the defining feature and primary driver of disease burden. A large European study of >500 European patients with PN described the itch as disturbing, burdensome, and intractable, often leading to sleep disturbance, skin pain, anxiety, and depression. Patients frequently describe feeling as though they have lost control of their skin and, in many ways, their identity. Treatment aims to break the itch-scratch cycle and restore quality of life.
The Neuroimmune Connection
A growing body of research has reframed PN as a neuroimmune disorder, where dysregulation of both nerve signaling and immune pathways drives the disease process. This evolving understanding has transformed treatment strategies, moving away from traditional multimodal approaches combining topical therapies, systemic immunosuppressants, and phototherapy toward targeted interventions that address specific pathways.
While PN and AD share overlapping mechanisms, the two are biologically distinct. Approximately 39% of PN patients have comorbid atopic dermatitis, but PN is a separate entity with its own complex pathogenesis. Recognizing this distinction helps clinicians select appropriate therapies and set realistic expectations for disease course and management.
Emerging Therapies for Prurigo Nodularis
For years, PN management relied on non-specific therapies which provided transient or limited relief. The understanding of PN as a neuroinflammatory condition has led to the development and use of targeted biologic and small molecule therapies that address the underlying drivers of this disease.
Dupilumab, an IL-4 receptor alpha inhibitor, became the first FDA-approved treatment for prurigo nodularis in September 2022. Treatment with dupilumab leads to significant improvement in itch, pain, and sleep as early as 2-3 weeks, with continued improvement in lesion clearance over time. The efficacy of dupilumab in PN is similar regardless of whether patients have an atopic background, and safety findings are similar to those observed in prior atopic dermatitis trials.
Nemolizumab, an IL-31 receptor inhibitor, offers another targeted approach by reducing both itch and skin pain. Its rapid onset of action and favorable short-term safety through 16 weeks make it an effective option for patients with PN.
Additional therapies, most notably JAK inhibitors such as topical ruxolitinib and povorcitinib, are under investigation and may further expand the therapeutic landscape for PN in the coming years.
Why PN Matters
PN’s impact extends far beyond the skin. The combination of unrelenting itch, visible scarring, and pigmentary changes can profoundly affect mental health and social well-being. PN is often underrecognized, particularly in patients with skin of color, where hyperpigmentation and lichenification may obscure the diagnosis or lead to misclassification as other dermatoses. Biologic therapies like dupilumab and nemolizumab are helping clinicians gain control of both itch and inflammation. These treatments not only improve symptoms but also represent a shift in how the dermatology community understands and manages PN.
Summary
-
- Prurigo nodularis is a distinct, neuroimmune-driven chronic disease, not merely a variant of atopic dermatitis.
- Clinicians should maintain a high index of suspicion for PN in patients presenting with chronic itch and nodular lesions, particularly in those with skin of color.
- Emerging biologic therapies have shown efficacy in safely treating patients with PN, and emerging treatments have the potential to further our understanding of the pathophysiology of this disease.
This information was presented at the 2025 Skin of Color Update conference by Raj J. Chovativa, MD, PhD, MSCI, FAAD. The above highlights from this lecture were written and compiled by Riyad N.H. Seervai, MD, PhD.