
Artificial intelligence (AI) is rapidly changing dermatology, and combining AI with dermoscopy is promising unprecedented diagnostic precision. However, as these technologies advance, a critical question remains: Are they designed to serve all patients equally?
Current diagnostic tools often underperform in patients with skin of color due to biases in training data and a lack of standardized imaging protocols. A poster presented at Skin of Color Update titled “Standardizing Pigment-Specific Dermoscopic and AI-Based Diagnostic Tools to Address Racial Disparities in Dermatology”, proposes a new framework to standardize pigment-specific dermoscopy and AI tools. I interviewed lead author Zahraa Rabeeah, MD, of the Boston University Department of Dermatology, to discuss how these innovations can bridge the gap in diagnostic equity.
What motivated you to explore pigment-specific dermoscopy & AI?
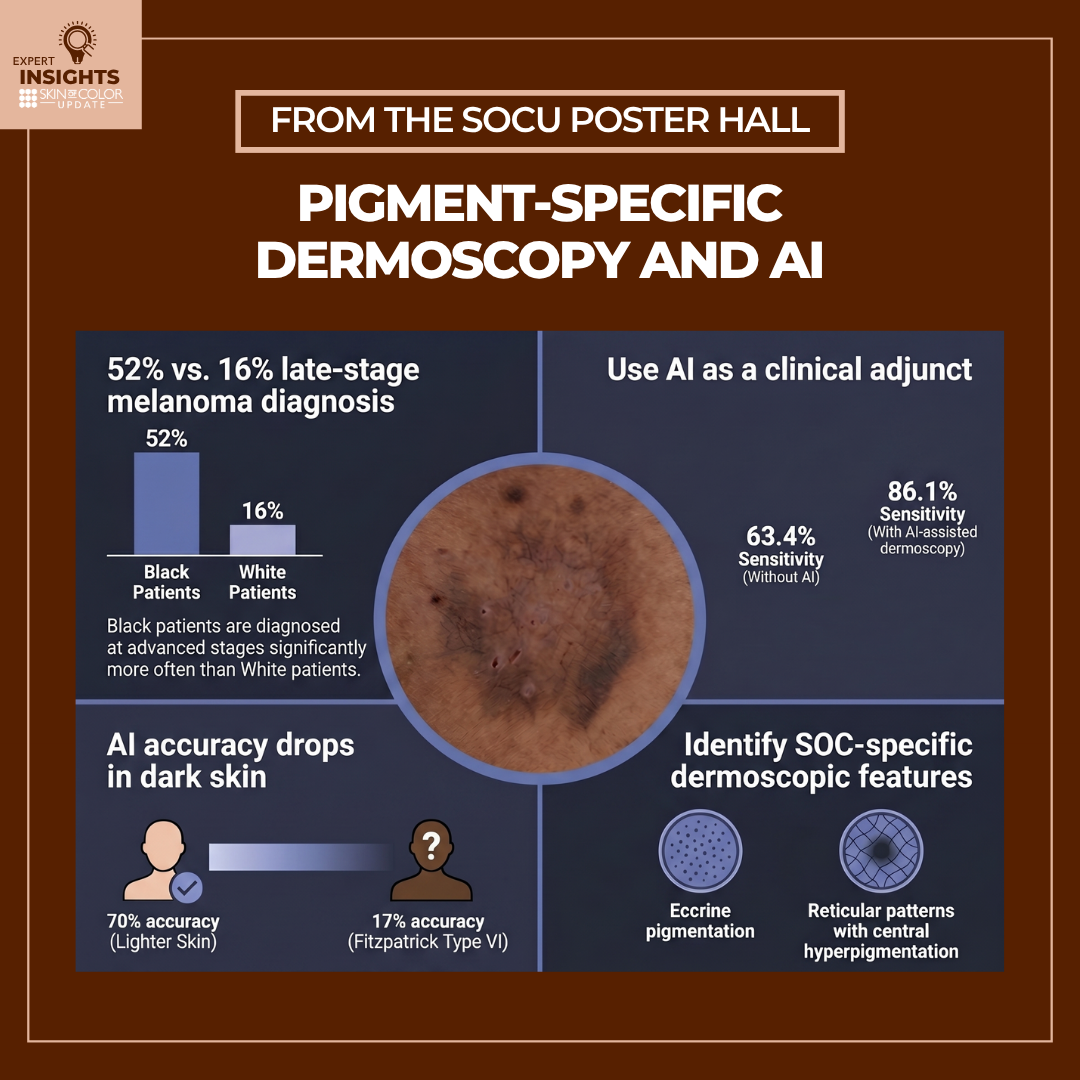
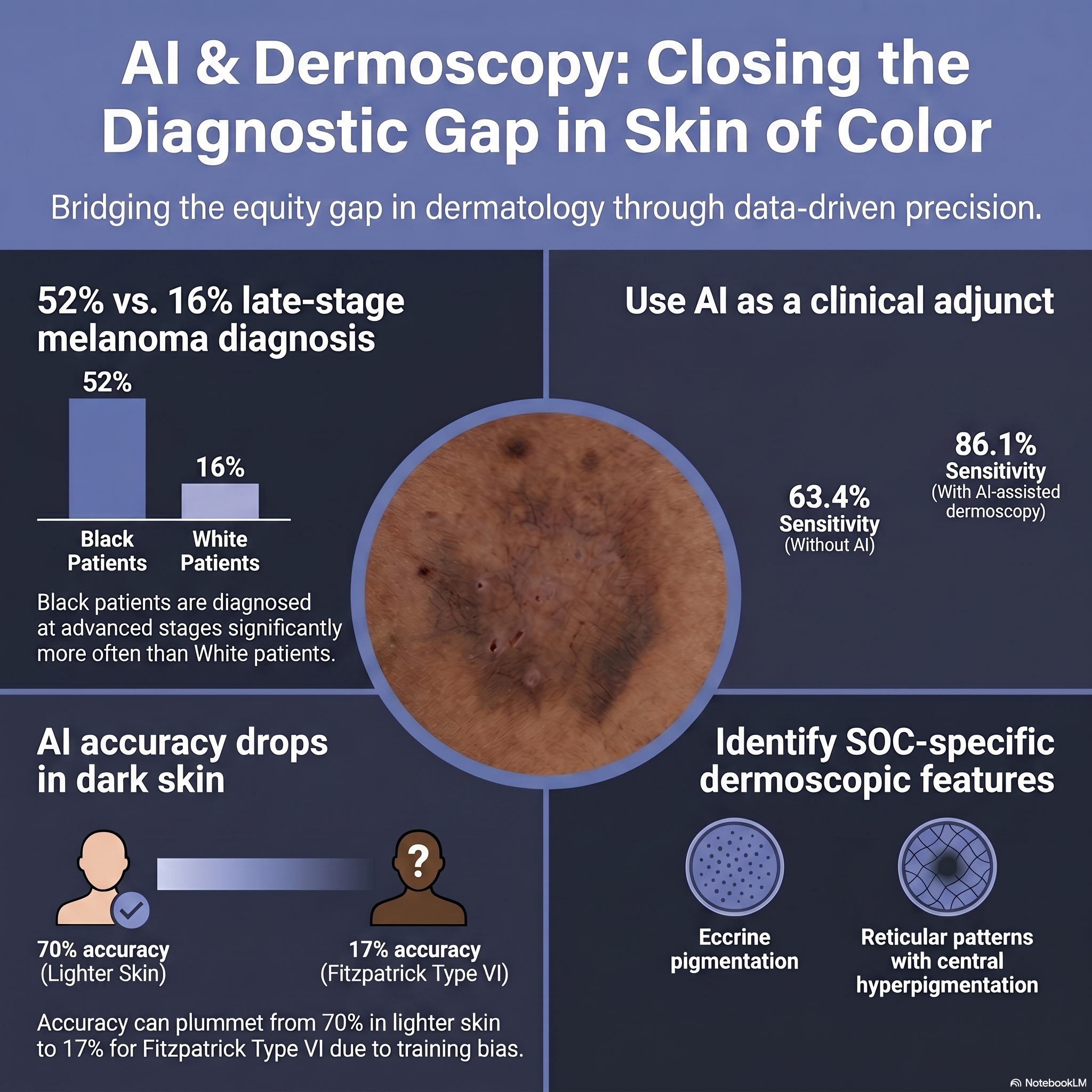
As clinicians, we are driven by a commitment to equitable care, yet we face a sobering reality in our daily practice: the “diagnostic gap.” Our motivation stems from the urgent clinical need to address the disparity where melanoma is diagnosed at a late stage in 52% of our Black patients, compared to only 16% of White patients. We know that inflammation and malignancy present differently in Fitzpatrick skin types V and VI—often lacking the “classic” erythema or patterns we were trained to spot in lighter skin. We wanted to evaluate whether standardizing pigment-specific dermoscopy and integrating AI support could serve as the equalizer we need to reduce morbidity and mortality in these populations.
How did you conduct your review, and what were you looking for?
We conducted a focused evidence-based review to evaluate the clinical utility of current diagnostic technologies. We weren’t just looking for theoretical potential; we were looking for actionable data.
Our search prioritized:
-
- Validation Studies: Data on sensitivity and specificity of dermoscopic criteria specifically in skin of color (SOC).
- Algorithm Performance: Real-world accuracy of CNNs (Convolutional Neural Networks) across diverse datasets.
- Workflow Feasibility: How these tools can be practically integrated into the busy workflows of outpatient clinics and primary care settings.
What did you discover?
We discovered a significant dichotomy: while AI and dermoscopy are powerful diagnostic adjuncts, “off-the-shelf” tools currently harbor dangerous biases if used uncritically.
-
- The “blind spot” in algorithms: Standard AI tools can perform well on lighter skin (approx. 70% accuracy) but can drop to as low as 17% accuracy for Fitzpatrick Type VI due to training data bias.
- The added clinical value: Despite this, when AI is optimized and paired with high-quality dermoscopy, it works. One study showed diagnostic sensitivity jumping from 63.4% (clinical exam alone) to 86.1% when using AI-assisted digital dermoscopy.
- New clinical pearls: We confirmed that “standard” dermoscopy rules don’t always apply. You must look for SOC-specific features—such as eccrine pigmentation and reticular patterns with central hyperpigmentation—to improve diagnostic yield.
Are these integrations occurring only in the research space or are some currently utilized in clinical practice?
While high-level integrated diagnostic systems are largely in the research or validation phase (e.g., DDI-AI devices), we are seeing immediate utility in telemedicine and triage.
For providers in primary care or resource-limited settings, AI-driven mobile health platforms (like those used effectively in global health initiatives) are beginning to support triage decisions. However, for routine high-level diagnostics in U.S. clinics, widespread adoption is currently limited by the need for standardization and EMR integration.
What’s needed in order to fully implement these integrations?
To bring this safely into your exam room, we need to address three critical clinical hurdles:
-
- Standardized Image Acquisition: AI is only as good as the input. We need uniform protocols for lighting, magnification, and angles in the clinic to ensure high quality input.
- Representative Datasets: We must demand that the tools we purchase are trained on diverse skin types. Current textbooks and datasets are overwhelmingly skewed toward lighter skin, which introduces liability and clinical risk.
- “Glass Box” AI: We need explainable AI. As the clinician is liable for the diagnosis, you need to know why the algorithm flagged a lesion, rather than relying on a “black box” output.
How could findings from this and subsequent studies transform patient care?
For the practicing clinician, these tools facilitate a shift from subjective assessment to objective, data-driven diagnosis. This transition offers:
-
- Risk Reduction: It offers a safety net to reduce the 62% misdiagnosis rate reported in some studies for melanoma in Black patients.
- Earlier Intervention: It moves the needle from reactive, late-stage management to proactive, early-stage detection, directly improving survival rates.
- Empowerment: It equips non-dermatology specialists with decision-support tools to triage pigmented lesions more confidently, reducing unnecessary referrals while catching the “can’t miss” diagnoses.
Is there anything else dermatology clinicians should know about pigment-specific dermoscopy & AI?
AI is an adjunct, not a replacement for your physical exam. Our review reinforces that algorithms cannot replace the tactile and contextual nuance of a skilled provider. AI cannot elicit a Darier’s sign or a buttonhole sign, nor can it fully interpret patient history.
The takeaway is not to wait for the technology to save us, but to actively upskill now: Familiarize yourself with pigment-specific dermoscopic patterns for skin of color and view AI as a “second opinion” to enhance, not replace, your clinical judgment.
Additional authors of the poster include:
Neena Edupuganti, DO, Department of Medicine, Piedmont Healthcare
Chinecherem Chime-Eze, MD, MPH, Department of Pediatrics, University of North Carolina at Chapel Hill
Nina Mbonu, MD, MHS, Department of Medicine, University of Tennessee Health Science Center
Chavely Calderon Casellas BS, Department of Dermatology, Boston University
Kelly Frasier, DO, MS, Department of Dermatology, Northwell Health
Alina G. Bridges, DO, Department of Dermatology, Northwell Health
Did you enjoy this scientific poster interview? You can find more here.