
Slate recently published a first-person account of fibrosing alopecia in a pattern direction (FAPD) in the article, “I’m 25, and I Have a Cosmetic Problem That No One Wants – and That’s Maddening to Fix.” The article details the writer’s years-long experience with hair thinning, and how it took until an irregular blood test and scalp biopsy for an FAPD diagnosis. The writer’s treatment includes a “kitchen sink” of therapies, and as with other forms of hair loss, FAPD often impacts the writer’s self-esteem. FAPD is only recently understood as a unique form of scarring hair loss.
For expertise in diagnosing and treating FAPD, I interviewed Amy McMichael, MD, FAAD, professor of dermatology at Wake Forest University School of Medicine. Dr. McMichael is co-chair of the upcoming Hair and Scalp Disorders: The Rx Pad and Beyond virtual conference.
As mentioned in the article, FAPD is a newly recognized condition. Have you diagnosed FAPD in your practice? If so, what were the signs and symptoms?
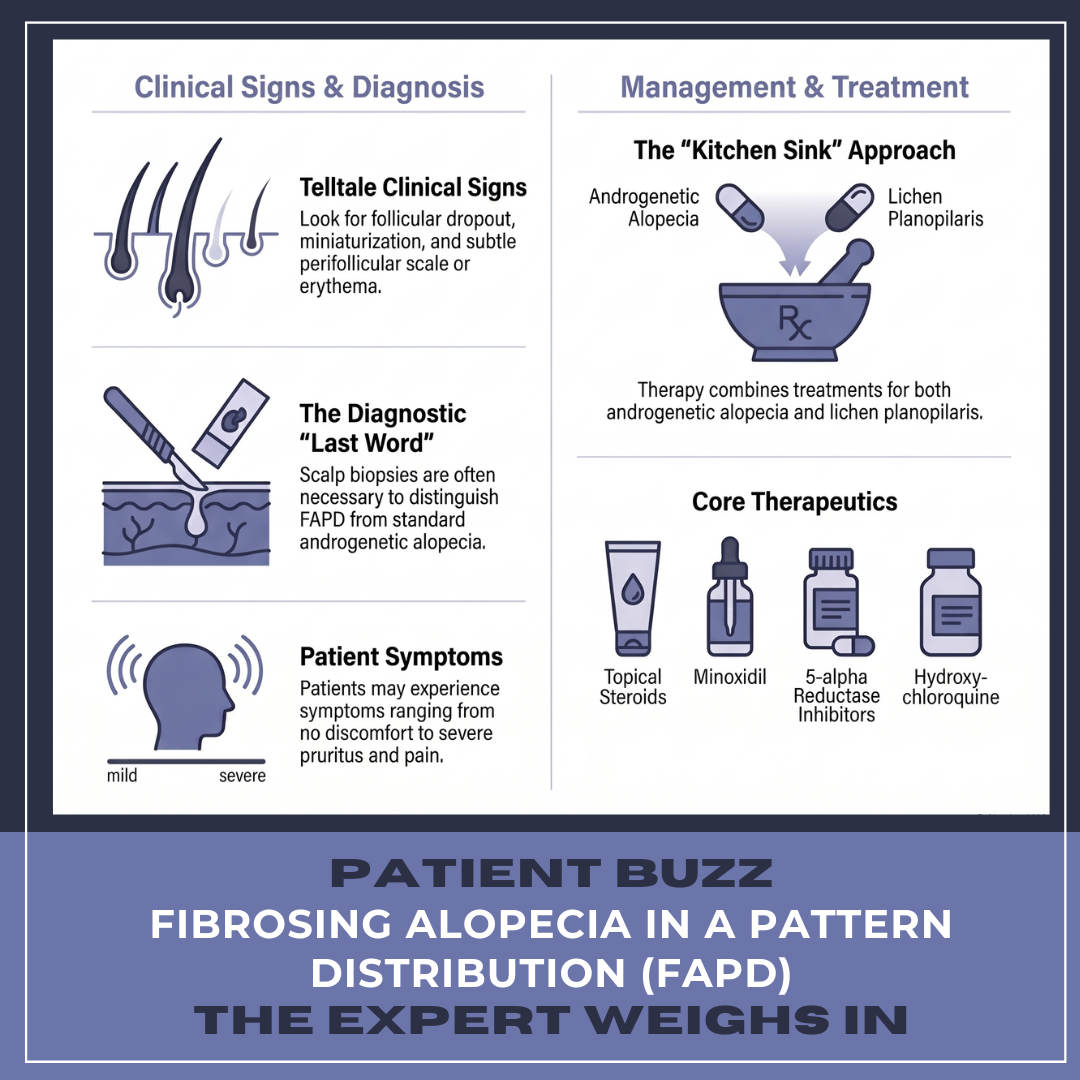
Yes, I have diagnosed many patients with FAPD in my practice. The typical appearance is a very similar clinical exam to that of female pattern hair loss. The telltale signs are follicular drop out on trichoscopy. Often there is a hint of perifollicular scale or erythema. Finally, at times, the only way to reliably diagnose FAPD is to perform a scalp biopsy.
What are the subtle “red flag” clinical signs that should prompt a dermatologist to look beyond a standard AGA diagnosis?
Subtle signs of FAPD include: perifollicular erythema, perifollicular scaling, follicular dropout, in addition to miniaturization.
What’s the role of scalp biopsy in diagnosing FAPD, and what considerations, such as the ideal site, should dermatologists keep in mind for an accurate diagnosis?
The scalp biopsy is often the last word on the diagnosis of FAPD. This diagnosis must be considered in order to not miss it. However, at times, the clinical signs are so subtle that a biopsy is necessary to tell this diagnosis from typical androgenetic alopecia. If the typical lymphocytic infiltrate along the basal layer with vacuolar interface change is not seen, even the biopsy may not help. Scarring with miniaturization should give the suspicion of FAPD, and clinical-pathologic correlation can be helpful.
Patients may also report burning, itching, or dysesthesia. To what extent should a patient’s discomfort influence the diagnosis?
Patients with FAPD can have everything from no symptoms to very severe pruritus and pain in the scalp. Often there is tenderness in affected areas of the scalp that are most affected, but some patients will have pain and tenderness, even when there are no signs of inflammation.
In which patient groups is FAPD most common? Does the incidence point to possible causes?
We see this condition in all races and ethnicities. At this point, we do not have full epidemiologic information for this disorder. We can say that most patients are women and adults. I have not seen this form of hair loss in children.
In the article, Dr. Alessandra Haskin says treatment essentially means using a kitchen sink of treatments with the hopes of success. What treatments have you found most effective for FAPD?
Essentially we use everything that works for androgenetic alopecia and lichen planopilaris. So this includes topical steroids, 5-alpha reductase inhibitors, minoxidil, hydroxychloroquine, followed by other anti-inflammatory systemic medications.
What do you think is the future of FAPD treatment?
Since this a form of lichen planopilaris, we will have better treatments when we crack the code on LLP.
Join Dr. McMichael on Saturday, June 27, for Hair and Scalp Disorders: The Rx Pad and Beyond, a complimentary, virtual, one-day conference. Dr. McMichael and Dr. Adam Friedman lead this full-spectrum perspective on hair and scalp management, from diagnosis to therapeutics to nutrition and lifestyle factors. Every session emphasizes practical tools, decision-making, and real-world implementation. Register today!
Did you enjoy this article? Find more Patient Buzz Expert Commentaries here.