
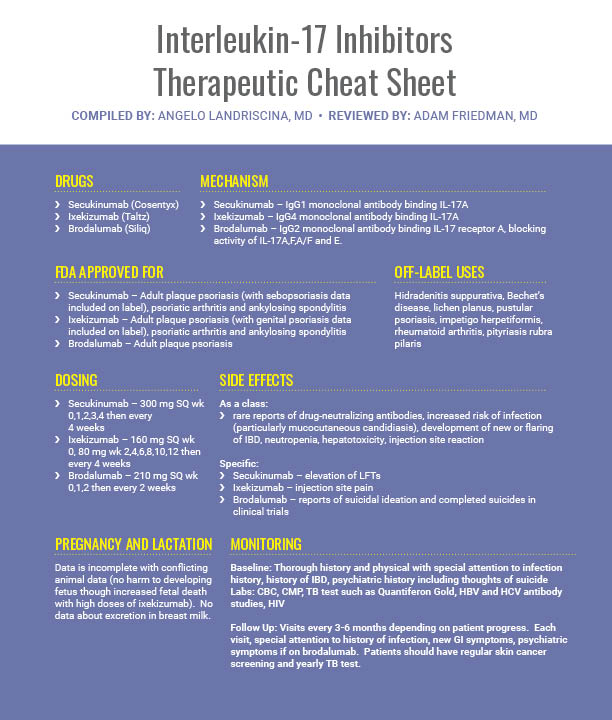
Biologics have revolutionized the treatment of psoriasis, and with new entries into the class, PASI90 and 100 have become attainable for many patients. In this installment of our Therapeutic Cheat Sheet series, we’ll cover everything you need to know to start and monitor your patients on IL-17 blocking therapies.
Further Reading
BACKGROUND: Secukinumab, a human monoclonal antibody that selectively targets interleukin-17A, is highly efficacious in the treatment of moderate-to-severe psoriasis, starting at early time points, with a sustained effect and a favorable safety profile. METHODS: Patients with moderate-to-severe plaque psoriasis were randomized to secukinumab 300 mg, secukinumab 150 mg, or placebo self-administered by prefilled syringe at baseline, weeks 1, 2, and 3, and then every four weeks from week 4 to 48. Efficacy responses (≥ 75/90/100% improvement in Psoriasis Area and Severity Index [PASI 75/90/100] and clear/almost clear skin by Investigator’s Global Assessment 2011 modified version [IGA mod 2011 0/1]) were measured to week 52. Patient-reported usability of the prefilled syringe was evaluated by the Self-Injection Assessment Questionnaire to week 48. RESULTS: The efficacy of secukinumab increased to week 16 and was maintained to week 52. With secukinumab 300 mg at week 52, PASI 75/90/100 and IGA mod 2011 0/1 responses were achieved by 83.5%/68.0%/47.5% and 71.5% of patients when analyzed by multiple imputation, respectively, and by 75.9%/62.1%/43.1% and 63.8% of patients when analyzed by nonresponder imputation, respectively. With secukinumab 150 mg at week 52, PASI 75/90/100 and IGA mod 2011 0/1 responses were achieved by 63.5%/50.3%/31.1% and 43.6% of patients when analyzed by multiple imputation, respectively, and by 61.0%/49.2%/30.5% and 42.4% of patients when analyzed by nonresponder imputation, respectively. Self-reported acceptability of the prefilled syringe was high throughout the study. The incidence of adverse events (AE) was well balanced between groups, with AEs reported in 74.4% of patients receiving secukinumab 300 mg and 77.3% of patients receiving secukinumab 150 mg. Nasopharyngitis was the most common AE across both secukinumab groups. CONCLUSION: Self-administration of secukinumab by prefilled syringe was associated with robust and sustained efficacy and a favorable safety profile up to week 52.
BACKGROUND: Newer psoriasis treatments can achieve greater levels of effcacy than older systemic therapies; however, current pso-riasis costs are substantial. We sought to estimate costs per additional responder associated with ixekizumab and etanercept, versus placebo, using effcacy data from phase 3 clinical trials (UNCOVER-2 and UNCOVER-3).
METHODS: In UNCOVER-2/UNCOVER-3, patients received subcutaneous placebo, etanercept 50 mg twice weekly (BIW), or ixekizumab one 80 mg injection every 2 weeks (Q2W) after a 160-mg starting dose. Twelve-week induction-phase Psoriasis Area and Severity Index (PASI) 75, PASI 90, and PASI 100 response rates for ixekizumab, etanercept, and placebo were obtained from pooled data from the overall and United States (US) subgroup intention-to-treat (ITT) populations, and used to calculate numbers needed to treat (NNTs) to achieve one additional PASI 75, PASI 90, or PASI 100 response for ixekizumab Q2W and etanercept BIW versus placebo. Twelve-week drug costs per patient were calculated based on the UNCOVER-2/UNCOVER-3 dosing schedule and wholesale acquisition costs. Mean costs per additional responder for PASI 75, PASI 90, and PASI 100 for each treatment versus placebo were calculated for pooled UN-COVER-2/UNCOVER-3 overall and US subgroup ITT populations.
RESULTS: Pooled overall ITT population: costs per additional PASI 75, PASI 90, or PASI 100 responder were US $37,540, US $46,299, or US $80,710 for ixekizumab Q2W and US $57,533, US $120,720, or US $404,695 for etanercept BIW, respectively. US subgroup ITT population: costs per additional PASI 75, PASI 90, or PASI 100 responder were US $38,165, US $49,740, or US $93,536 for ixekizumab Q2W and US $69,580, US $140,881, or US $631,875 for etanercept BIW, respectively.
CONCLUSIONS: Twelve-week costs per additional responder were lower for ixekizumab Q2W than for etanercept BIW across all levels of clearance (PASI 75, PASI 90, and PASI 100) in the pooled UNCOVER-2/UNCOVER-3 overall and US subgroup ITT populations.
![]() Treatment of Recalcitrant Acrodermatitis Continua of Hallopeau With Brodalumab – CASE REPORT
Treatment of Recalcitrant Acrodermatitis Continua of Hallopeau With Brodalumab – CASE REPORT
Acrodermatitis continua of Hallopeau (ACH) is a relatively rare chronic disorder with clinical findings of pustules and erythematous plaques on the digits.1 Although it is a variant of pustular psoriasis, it can be resistant to multiple lines of therapy. We describe for the first time a patient with recalcitrant ACH successfully treated with brodalumab, an interleukin-17 receptor A (IL-17RA) blocking antibody.
Did you enjoy this Therapeutic Cheat Sheet? You can find more here.
Next Steps in Derm is brought to you by SanovaWorks.