
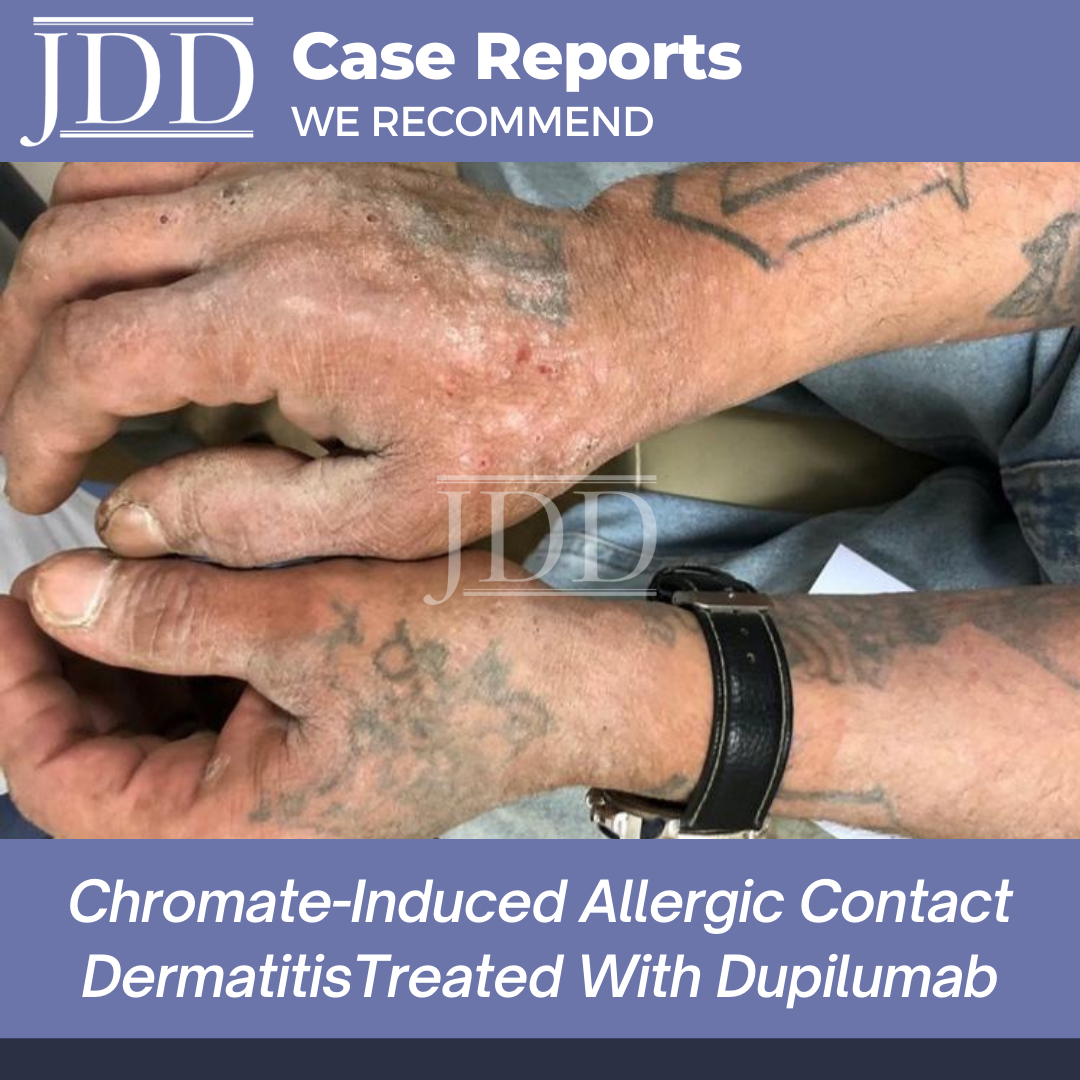
Chromate causes persistent, difficult to treat irritant and allergic contact dermatitis in cement-handling occupational workers. When therapeutics such as topical corticosteroids, topical calcineurin inhibitors, phototherapy and immune-modulating treatments like methotrexate fail, many patients are advised that avoidance may be the only remaining option – an option that may be particularly challenging if the patient’s occupation necessitates chromate exposure. JDD authors Britney N. Wilson MBS, Esther A. Balogh MD, David J. Rayhan MD, Paul K. Shitabata MD, Daniel J. Yousefzadeh BA, and Steven R. Feldman MD PhD, rereport a case of severe chromate-induced allergic contact dermatitis in a 55-year-old cement mason that presented to the outpatient dermatology clinic with multiple scaly, erythematous, >5 cm plaques scattered over the skin of his hands, head and neck. After a prior failed course of treatment with high potency topical corticosteroid, this patient was successfully treated with dupilumab. Given the success of dupilumab in their patient, the authors propose the consideration of dupilumab as an alternative treatment option for those suffering from chromate-induced allergic contact dermatitis that is refractory to ultra-high potency topical corticosteroids.
Introduction
Case

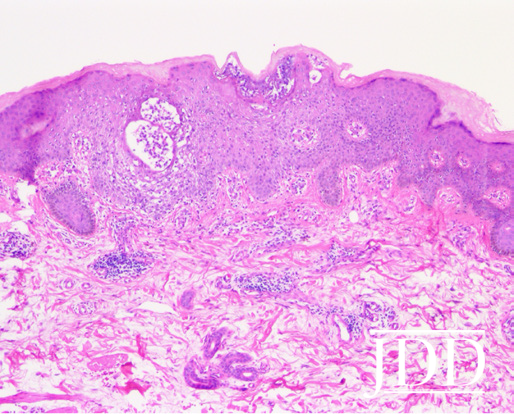
right ventral forearm. There are spongiotic vesicles in the epidermis
and a superficial mononuclear perivascular infiltrate (4x magnification).
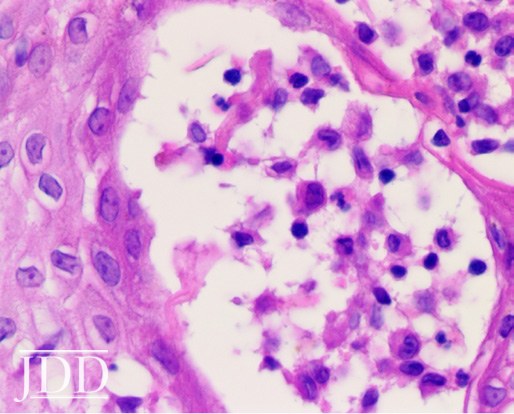
spongiotic vesicles in the epidermis contain mononuclear cells (40x
magnification).
Given the frank presentation and history of dermatitis only in areas where the patient was exposed to cement dust, the patient was not patch tested for chromium. Because he had not shown any clinical improvement in the past with ultra-high potency topical steroids, topical therapy was not reattempted. Due to his past history of viral hepatitis, methotrexate was considered but ultimately not pursued as a treatment option. Consequently, the patient was started on dupilumab, and received one loading dose of 600 mg. After a misinterpretation of the recommended dosing, the patient continued the 600 mg dose every two weeks for 2 months, at which time he presented for a follow up visit at which his dupilumab dose was decreased to 300 mg every two weeks. At that point, the patient’s dermatitis had completely resolved (Figure 4), and he reported no adverse events (and, in particular, no conjunctivitis) throughout the treatment course. Though the patient’s occupational exposure to chromate as a cement mason did not change, the patient’s dermatitis remained clear for the next 18 months to date (July 2020).

one year of treatment with dupilumab.
Discussion
Clinically, chromate allergy appears as a severe, sometimes widespread, very persistent dermatitis, and is considered to have a relatively poor prognosis, often with therapeutic recalcitrance.7 Commonly used treatments for chromate induced ACD include emollients, topical corticosteroids, and topical calcineurin inhibitors.
Treatments for persistent or severe chromate-induced contact dermatitis include phototherapy and immune-modulating treatments such as azathioprine, cyclosporin and methotrexate. Until recently, when these options failed, avoidance was the only long-term management strategy available, often with negative ramifications on the livelihoods of patients who are occupationally exposed to chromate.
The case we present provides a novel treatment approach for a rare form of ACD that has the ability to significantly impact the quality of life of those affected. Dupilumab is commonly used in the treatment of atopic dermatitis (AD), a helper T-cell 2 (TH2) axis-predominant immune disorder. Dupilumab acts as an IL-4 receptor antagonist and prevents the IL-4 and IL-13- mediated inflammatory responses seen in AD. Although ACD is considered predominantly a helper T-cell 1 (TH1)-mediated process, certain allergens sensitize via the induction of the TH2 pathways.8,9 Dupilumab may be effective in the inhibition of allergens that elicit a TH2-mediated, IL-4 dependent ACD.8The ability of dupilumab to treat chromate-induced ACD in our patient also suggests that IL-4 or IL-13 may play a role in ACD. The role of IL-4 in ACD was confirmed in IL-4 knockout mice, which still have the ability to elicit contact sensitivities to oxazolone but not 2,4,6-trinitrochlorobenzene, a contact allergen with a TH2-mediated sensitization pathway.8,10Dupilumab may be an alternative treatment option for those suffering from chromiuminduced ACD that is recalcitrant to even ultra-high potency topical corticosteroids.
Disclosures
References
2. Wilbur S, Abadin H, Fay M, Yu D, Tencza B, Ingerman L et al. Agency for Toxic Substances and Disease Registry (ATSDR) Toxicological Profiles. Toxicological Profile for Chromium. Atlanta (GA): Agency for Toxic Substances and Disease Registry (US); 2012.
3. Sharma AD. Low chromate diet in dermatology. Indian J Dermatol. 2009;54:293-5.
4. Buters J , Biedermann T. Chromium(VI) Contact Dermatitis: Getting Closer to Understanding the Underlying Mechanisms of Toxicity and Sensitization! J Invest Dermatol. 2017;137:274-7.
5. Costa M , Klein CB. Toxicity and carcinogenicity of chromium compounds in humans. Crit Rev Toxicol. 2006;36:155-63.
6. Bruynzeel DP, Diepgen TL, Andersen KE, Brandao FM, Bruze M, Frosch PJ et al. Monitoring the European standard series in 10 centres 1996-2000. Contact Derm. 2005;53:146-9.
7. Bregnbak D, Thyssen JP, Zachariae C , Johansen JD. Characteristics of chromium-allergic dermatitis patients prior to regulatory intervention for chromium in leather: a questionnaire study. Contact Derm. 2014;71:338-47.
8. Machler BC, Sung CT, Darwin E , Jacob SE. Dupilumab use in allergic contact dermatitis. J Am Acad Dermatol. 2019;80:280-1.e1.
9. Kohli N , Nedorost S. Inflamed skin predisposes to sensitization to less potent allergens. J Am Acad Dermatol. 2016;75:312-7.e1.
10. Dieli F, Sireci G, Scire E, Salerno A , Bellavia A. Impaired contact hypersensitivity to trinitrochlorobenzene in interleukin-4-deficient mice. J Immunol. 1999;98:71-9.
Source
Content and images used with permission from the Journal of Drugs in Dermatology.
Adapted from original article for length and style.