
Children with dermatologic conditions, ranging from eczema to psoriasis to hidradenitis suppurativa, are benefitting from advances in biologic therapy with several FDA-approved treatment options. However, real-life clinical experience reveals biologic therapy is not always initiated when prescribed. In addition, even when biologic therapy is initiated, adherence is often not maintained. Therefore, the benefits of biologics may not be fully realized in this patient population.
An ODAC poster explores the frequency of biologic non-initiation and non-adherence in children — as well as reasons for non-compliance — using data from Children’s National Hospital in Washington, D.C. I interviewed poster author Jared Kupersmith, BS, a medical student at the George Washington University School of Medicine and Health Sciences conducting research at the Children’s National Hospital Department of Dermatology.
What motivated you to investigate biologic adherence in children?
I worked as a medical assistant in a dermatology clinic before attending medical school, and one of my main responsibilities was to work with both the physicians and insurance companies to get prior authorizations approved and patients set up with resources to start their biologic therapies. However, the patients were frequently coming back for their follow-up visits having stopped their medication, or never even started therapy. Having seen many patients experience life-changing improvements in their conditions with the use of biologics, I became motivated to investigate the true scope of the problem, as well as the factors driving the seemingly low rates of adherence to therapy, particularly among children.
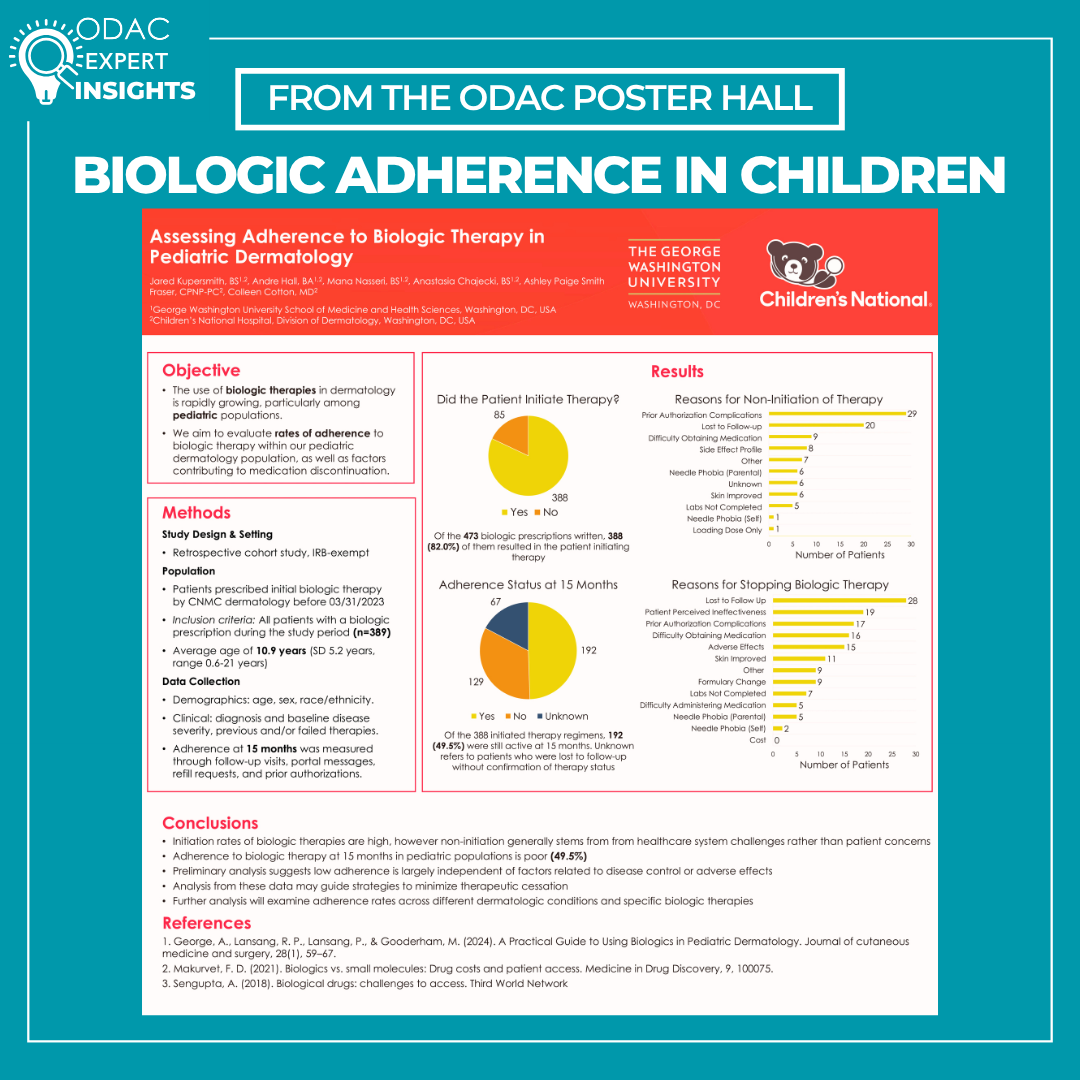
You looked at initiation as well as adherence at 15 months among Children’s National Hospital dermatology patients who were prescribed a biologic. What percentage of patients who were prescribed a biologic initiated therapy and what percentage of those initiated prescriptions were still active after 15 months?
There were 389 patients in our population, with 473 biologic prescriptions written. Of those 473 prescriptions, 388 of them (82.0%) resulted in the patient initiating therapy. At 15 months, only 192 (49.5%) of those initiated prescriptions were still active.
What were some of the reasons for nonadherence, and how did they differ from initiation to the 15-month mark?
The most common reasons for non-initiation were prior authorization complications (n=29), patients being lost to follow-up (n=20), and difficulty obtaining medication from the specialty pharmacy (n=9). In contrast, the most common reasons for non-adherence at 15 months were patients being lost to follow-up (n=28), patients perceiving ineffectiveness of therapy (n=19), and prior authorization complications (n=17).
Did the results of your study confirm your hypothesis? Were any of the results surprising?
These results have confirmed our hypothesis that adherence to biologic therapy at 15 months in pediatric populations is poor. Many of the reasons driving this trend revolve around challenges faced by patients in the healthcare system, rather than concerns with the medications themselves. One set of results that was surprising was the low reported rates of discontinuation of medication due to the child experiencing needle phobia. All biologic medications must be given as subcutaneous injections, sometimes as frequently as once weekly. In our population, only one patient did not initiate therapy, and two patients discontinued therapy by 15 months due to the child experiencing needle phobia. Our pediatric dermatology clinic enjoys a relationship with a psychologist who works with children with needle phobia, which could account for the low occurrence of this issue.
What does this tell clinicians and medical systems about barriers to biologic care? What needs to change for patients to receive the care they are prescribed?
These findings highlight that the major barriers to biologic care are systemic rather than clinical. Prior authorization complications remain a dominant obstacle to both initiating and sustaining therapy, underscoring how insurance processes can delay or derail evidence-based treatment. The high rate of patients being lost to follow-up suggests gaps in care continuity, patient navigation, and support infrastructure. Together, these data indicate that improving access to biologics will require streamlined authorization processes, better coordination with specialty pharmacies, proactive follow-up systems, and enhanced patient engagement to ensure patients can start, continue, and benefit from the therapies they are prescribed.
What else should dermatology clinicians know about biologic adherence in children?
A smaller, but still significant portion of the children who did not initiate therapy indicated their reasoning to be the side effect profile of these medications (n=8). Many of the biologic medications, including dupilumab ,which is approved for children as young as six months old, have a long list of possible side effects reported on the label. In the age of artificial intelligence and easy access to information, patients (and their parents) can easily find these lists and become overwhelmed and uneasy about the medication. In practice, many such side effects are rare or not applicable to the pediatric population. Therefore, counseling patients appropriately on the relative risks of these medications at their initial appointment balanced with the risk of undertreated skin disease is important to both obtain informed consent while putting any fears at ease.
Additional authors of the poster include:
Andre Hall, BA, George Washington University School of Medicine and Health Sciences, and Children’s National Hospital, Division of Dermatology
Mana Nasseri, BS, George Washington University School of Medicine and Health Sciences, and Children’s National Hospital, Division of Dermatology
Anastasia Chajecki, BS, George Washington University School of Medicine and Health Sciences, and Children’s National Hospital, Division of Dermatology
Ashley Paige Smith Fraser, CPNP-PC, Children’s National Hospital, Division of Dermatology
Colleen Cotton, MD, Children’s National Hospital, Division of Dermatology
Did you enjoy this scientific poster interview? You can find more here.